Understanding Sexual Health
Sexual Desire
Sexual Arousal
Sexual Orgasm
Intercourse Pain
Other Sexual Issues
Self-care & Natural Remedies
Therapy & Treatments
Therapy Sexual Desire
Therapy Sexual Arousal
Therapy Sexual Orgasm
Therapy Intercourse Pain
Therapy Vaginal Dryness
Understanding Sexual Health & Menopause Sexuality
Sexuality is a fundamental part of the human experience that relates to the sexual habits and desires of a person. Sexuality is a very personal characteristic. It is difficult to determine what is or is not ‘normal’ for an individual because every person has their own definition based on individual culture, background, personal sexual experiences, and biology. Even the World Health Organization can’t provide a specific, non-subjective definition! They define sexual health as a state of physical, emotional, mental and social well-being related to sexuality; it is not merely the absence of disease, dysfunction or infirmity.
Despite the variability in definitions, there are a few basic concepts that are required for an individual’s healthy sexual response and function. They are:
- comfort with their degree of desire for sex
- comfort with their ability to enjoy sex
- comfort with their levels of sexual desire, response, and function
Physiological, psychological, social and emotional factors can all be involved in problems with sexuality.

Female Sexual Dysfunction (FSD) has four formal categories: problems with desire, arousal, orgasm and pain. Research shows that 30-50% of peri- and postmenopausal women experience sexual problems in one or more of these areas.
Experiencing sexual problems is not the same thing as being bothered or distressed by them. Perimenopausal women report a much higher frequency of distressing sexual problems compared to post-menopausal women, even though the actual prevalence of sexual problems is lower. So during the menopausal transition, women have fewer sexual problems than post-menopausal women, but they are more distressed by them. [1]

Libido
Sexual libido is defined as interest in sex and in being sexual. It is usually the first phase of a sexual response. There are three elements to libido:
- Sexual drive (biological). Sex drive can be experienced as sexual thoughts and fantasies, actively looking for sexual activity, or tingling and sensitivity in the genitals. Sex drive is variable among women, and can vary individually as well, based on activity, levels of stress, and overall health.
- Personal attitudes (psychological). Your beliefs, values, and expectations can impact your natural sex drive. Your attitudes result from a combination of your culture, your religious beliefs, your personal history, and your family and friends. Typically, a positive attitude about sex results in greater sexual desire.
- Motivation (psychological / emotional / interpersonal). Motivation is your willingness to behave sexually with a particular partner at any particular time. Motivation is considered to be the most complex component of desire and many experts consider it to be the most important.
Desire is known to decline with age in both men and women, however women are two to three times more likely to be affected by a reduction in their perimenopause libido and their menopause libido. The effect of aging is variable – some women experience a menopause loss of libido beginning in their midlife years, others notice no change, and a few women in menopause have increased libido. Increased interest may be a result of freedom from contraception (once they hit menopause) or by the increased privacy they experience once their children (if they have any) leave home. While hormones may reduce episodes of spontaneous desire (the mental interest in having sex before there is any stimulus), receptive desire (interest in having sex when your partner initiates it) doesn’t seem to be affected in the same way. [2]

Arousal
Arousal is the physical process that readies your body for sex. Blood flow to the genitals increases, the vaginal lining becomes lubricated, breathing and heart rate speed up, muscles tense, and nipples become erect. Sexual desire usually triggers arousal, but as women age and move through the menopausal transition, sex drive can shift from being the first phase of their sexual response and instead, it becomes the second phase, following arousal. This is commonly seen when your partner initiates sex with seduction or suggestion and then you consciously respond.
Female arousal after menopause is affected by hormone levels. Lower levels of estrogen can lower the blood supply to the vagina and cause vaginal atrophy (atrophic vaginitis) – an awful name for a common issue. The tissues in the vagina weaken, get thinner, dryer, and may get inflamed, causing pain, burning, or discharge. In fact one of the first noticeable signs of the menopausal transition is reduced vaginal lubrication during arousal. When the vagina is dry, sex can be uncomfortable. Lowered blood supply also reduces circulation to the vulva, clitoris and the vagina, making arousal more difficult. [2] [3]

Orgasm
Changes in hormones and to the vagina, including reduced blood flow (especially to the clitoris), can impact a woman’s ability to achieve orgasm. The clitoris has an abundance of nerve endings and is extremely sensitive, making it the anatomical source of female sexual pleasure. During the menopausal transition, the clitoris can lose its sensitivity, in part from the reduction in estrogen levels but also due to age-related changes to the circulatory and nervous systems.
This means that sensations and pleasure felt during sex are reduced and they in turn cause changes to the experience of an orgasm in that they may take longer to achieve or be less intense. This is called female orgasmic disorder. Problems with orgasm are more common in women over the age of 45. [2]
There are two main types of orgasm problems – primary problems, where the woman has never achieved orgasm, or secondary problems where the lack of orgasm results from another sexual issue such as problems with desire or arousal. [9]

Dyspareunia or Painful Sex
The lower levels of estrogen seen during the menopausal transition may cause changes to your vaginal tissues – they get thinner, dryer, and may get inflamed, causing pain, burning, or discharge. When this happens, penetration and intercourse can become very uncomfortable or even severely painful. Sadly dyspareunia is not rare as between 17% and 45% of postmenopausal women say they find sex painful.

Other Sexual Health Factors
Sexuality is a highly personal and complex characteristic and many different factors can affect a woman’s interest in sex. While this is true at any point during a woman’s lifetime, the menopausal transition causes many changes in a woman’s life, many of which can influence her sexual health and sexuality. Other factors may influence a woman’s level of interest in sex during the menopausal transition and after, including
In addition to the direct impacts of depression and anxiety, treatment options for depression include selective serotonin reuptake inhibitors (SSRI) and serotonin and norepinephrine reuptake inhibitor (SNRI) antidepressant drugs. These have well-known negative impacts on desire and they can slow sexual response.
- Stress and feelings of being overwhelmed
- Other health concerns
- Normal changes associated with aging [3]
Self-care & Natural Remedies for Sexual Health
Adapting to changes in your sexuality and sexual health can be hard when you are processing the fact that your body is changing. However, your brain is one of your best sex organs! Because the basis of sexuality is so complex and individual, there are many steps you can take to accommodate any changes to your regular sex life, some of which may in fact lead to better and more satisfying sex. This can happen because when you have to start speaking openly and communicating about your sexuality, you may find that you are in a better position to ask for exactly what you need and want.
There are some basic steps you can take to improve your sexuality and adjust to any sexual changes. TALK! Talk to your partner. Tell them what is happening for you. They are part of your sexual experience, so they should also be part of your sexual solutions.

When you avoid sex it can have an impact on your partner and create stress in the relationship. When there is stress in the relationship, satisfying sex becomes more difficult to achieve. To manage this, try:
- Enjoy your time together! Make (and follow through on) plans for dates, seduction, and intimacy.
- Reduce your focus on sex and orgasm, and increase your focus on having fun and relaxing time together – enjoy foreplay, give or recieve massages, or try new variations of activities you have enjoyed. While orgasm is definitely nice to have, it doesn’t have to be the only thing that matters every time you have sex.
- Consider short-term couples counseling with a therapist, particularly one who specializes in sex therapy.
- If you are experiencing pain, ensure you are using vaginal lubricants (talk to your pharmacist or your healthcare provider and see the Therapy Section below).
- Focus on relaxing before intimacy with a bath or a meditation. Remember that it’s hard to stay in the moment when you are tensing up!
- If you are experiencing any discomfort at all, you may also consider trying new positions, including ones that allow you to control the depth of penetration.
- If you are comfortable, experiment with erotica and masturbation. Try new things!
If you do not have a partner, it is still normal and proper to be concerned about changes to your sexuality. TALK. Talk to trusted family or friends or your healthcare provider.
In some cases, women may have been experiencing unsatisfactory sex over the years and have found a way to cope. In other cases, women may not be comfortable being open about their needs and desires because they are embarrassed or ashamed of them. In these cases, the menopausal transition can be seen as a great opportunity to make changes. Women at mid-life have so much more experience than they had when they started having sex – they can now take advantage of their stronger voice and make the time to address hang-ups or mental blocks.
Despite how often women in the menopausal transition or postmenopause are troubled by sexual problems, most don’t discuss these problems with their healthcare providers. In fact, a survey of US women ages 57 to 85, showed that only 22% of women reported that they had discussed sex with a physician since they turned 50. [4] Talking to your healthcare provider should be a first step because, as with many health issues, women are in a position where they must advocate for themselves.
Sex can be a loaded topic because it is so affected by cultural and religious norms, but don’t forget, it is an important part of who you are – and you owe it to yourself to take care of your sexual health just as you would take care of any other health issue that is impacting you.
Therapy & Treatment for Sexual Health
At age 40 find a reliable, educated primary care provider familiar with recognizing and treating symptoms of perimenopause and menopause. The North American Menopause Society provides a list of menopause practitioners.
Lack of Desire / Low libido / Low Sex Drive
Although sexual problems can be hard to discuss, talk to your doctor. There are options for you to consider, such as counseling or new treatments such as a combination of estrogen and male hormones called androgens that researchers are studying to see if they effectively help boost sex drive in women.
Your doctor may refer you and your partner to a health professional who specializes in sexual dysfunction. The therapist may advise sexual counseling on an individual basis, with your partner, or in a support group. This type of counseling can be very successful, even when it’s done on a short-term basis.
Recall from the introductory section that sexual desire is usually the first sexual response and that desire triggers arousal. During the menopausal transition, sex drive can change from being the first phase of sexual response and instead, it becomes the second phase, following arousal. If you are experiencing problems with a lack of desire, it is worth experimenting with different ways to get aroused, as this may start your desire.
Arousal Problems
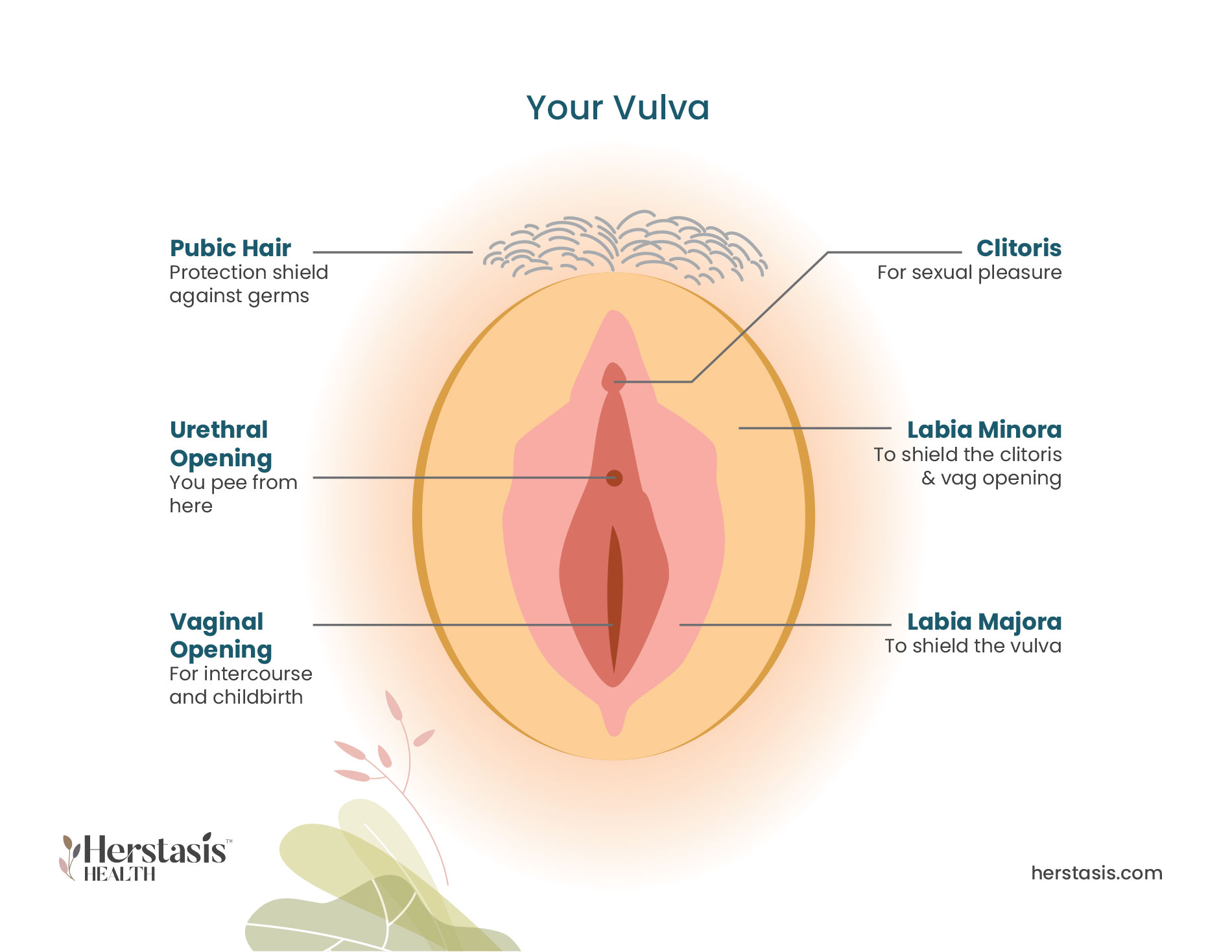
The clitoris, located above the opening of the vagina, is often called the primary source of female sexual pleasure due to its very high density of nerve endings. For the majority of women, arousal starts when the clitoris becomes engorged with blood. Treatment for arousal problems centers around increasing blood flow to the clitoris.
Your doctor can prescribe a sexual aid called the EROS clitoral therapy device (EROS-CTD) to help with this. EROS is the only FDA-approved mechanical device designed specifically to help with arousal problems. The device itself is a small battery-operated suction cup that gets placed over the clitoris before sex. A battery-operated vacuum pump provides suction to the clitoral area, drawing blood into the clitoris that results in increased pressure on the clitoral nerve. Research has shown that using this device increases lubrication, sensation, and even the number of orgasms in many women who have used it. [6] [7]

Orgasm Problems
Orgasm problems can be a primary disorder (where the woman has never achieved orgasm) or a secondary disorder (where the lack of orgasm results from another type of sexual dysfunction such as hypoactive sexual desire disorder or low sex drive). [9]
Primary orgasm problems may be genetic or may be the result of a history of trauma or abuse. It typically does not resolve without treatment. Individual and/or couples therapy may be able to help with orgasm problems if they stem from a past traumatic history. Unfortunately, there does not appear to be an effective therapy for unexplained primary orgasmic disorder in which the patient has never achieved orgasm, even through masturbation.
Secondary orgasmic disorder often resolves when the primary issue is treated. In the meantime, education about and practice with masturbation techniques may be helpful.

Vaginal Dryness
If your vaginal dryness is caused by low estrogen levels, your healthcare provider may prescribe topical estrogen therapy. There are three methods of applying vaginal estrogen:
- Ring: You or your doctor can insert a soft, flexible ring into your vagina. It releases estrogen directly to the vaginal tissues. The ring lasts about three months so it will need to be replaced regularly.
- Tablets: These tablets are inserted into your vagina with a disposable applicator.
- Cream: The cream is inserted into your vagina using an applicator.
There are over-the-counter vaginal moisturizers as well. Speak to your pharmacist or your healthcare provider to get a recommendation. Water-soluble lubricants (such as Astroglide or K-Y Jelly) can also be used on an as-needed basis. Non-water-soluble lubricants, such as Vaseline, are not recommended if you are using condoms for either contraception or for prevention of STIs because they can weaken latex and reduce the effectiveness of the condom. [5]
Avoid using douches, bubble baths, scented soaps, and lotions around your vaginal area. These products can make any existing dryness even worse.
Don’t forget that your brain is a sexual organ – take your time during arousal and make sure that you are relaxed. This easy step can reduce the ‘performance stress’ that can occur when you start to get stressed because it is taking time to get lubricated. This stress can start a vicious cycle of stress → dryness → more stress.
Sex Pain
The lower levels of estrogen seen during the menopausal transition can cause your vaginal tissues to get thinner, dryer, and they may get inflamed, causing pain, burning, or discharge. Some oral estrogens (estrogen therapy taken in a tablet that circulates the estrogen throughout your body to all tissues) can help vaginal tissue become thicker and less fragile, which will decrease the experience of pain.
Note that some oral estrogen hormone therapies are known to thicken the lining of the uterus (the endometrium) causing a condition known as endometrial hyperplasia that is usually associated with too little progesterone. Talk to your healthcare provider to find the best oral estrogen for your needs.
The Science
Information on how the menopausal transition interacts with your sexual health.
Understanding the Lack of Desire
Learn More
Understanding the Lack of Desire
The formal name for decreased or lowered desire is Hypoactive Sexual Desire Disorder. [9] Scientific studies have consistently shown that about one third of women in the US women report low sexual desire or interest. This lack of desire, however, is only troubling to about one in three of those women. [2] Midlife women, who are typically in the menopausal transition, report being troubled by their lack of desire at a higher rate (12% reporting) compared to both post-menopausal women (7% reporting) or women younger than 45 years of age (9%). [1]
One large (31,581 participants) cross-sectional, nationally representative study in the US is called the Prevalence of Female Sexual Problems Associated with Distress and Determinants of Treatment Seeking (PRESIDE) study. [8] This study used a 42 item questionnaire to measure sexual function, sexual distress, demographic, and health-related factors. The results showed that women with low sexual desire were most likely to be distressed by their lack of desire if they:
- are currently in a relationship with a partner
- are 35 to 64 years old (in midlife vs older or postmenopausal)
- are experiencing depression
Other factors also influenced whether women were bothered by their lack of desire, including urinary incontinence, anxiety, social skills, and the experience of other problems with arousal or orgasm. Women’s satisfaction about their overall relationship with their partner also had an important effect on desire and any distress they felt because of low desire. The study concluded that the strongest correlate of women being distressed about their lack of desire was having a current partner. In other words, women without a partner may experience a lack of desire but they are not as troubled by it. [8]
Although not directly related to menopause, an age-related decrease in testosterone may also play a role in reduced desire for midlife women. Testosterone is known to play a role in women’s sex drive and experiencing sexual sensation. The direct relationship between testosterone and sexual desire needs more research as low sexual desire in women does not appear to be related to testosterone levels in scientific studies. [2]
Understanding Arousal Problems
Learn More
Understanding Arousal Problems
Difficulties with arousal are formally classified as Female Sexual Arousal Disorder. Arousal difficulties can result from changing hormone levels, and are also often seen in women experiencing other gynecologic or chronic medical conditions. Certain antidepressant medications, particularly selective serotonin reuptake inhibitors (SSRI) and serotonin and norepinephrine reuptake inhibitors (SNRI) can have a negative impact on the ability to experience sexual arousal. Arousal issues usually resolve when the underlying condition is treated or the medication is adjusted.
The Prevalence of Female Sexual Problems Associated with Distress and Determinants of Treatment Seeking (PRESIDE) study reported that arousal problems that cause distress or concern affect about 5% of US women. In that survey, the rate of bothersome arousal problems was highest among women ages 45 to 64 (7.5%) compared to women 65 or older (6%) or women younger than 45 (3%). [8]
Additionally, this research showed that troublesome arousal problems are more common among women:
- who are married or living with their partner
- women who had experienced surgical (rather than natural) menopause. This occurs as a result of an oophorectomy, a surgery that removes the ovaries that are the main source of estrogen production in the female body.
- women who were in worse overall health. [8]
Understanding Orgasm Problems
Learn More
Understanding Orgasm Problems
A persistent or recurrent delay in, or total absence of orgasm after a normal arousal phase and adequate stimulation is called Female Orgasmic Disorder. It occurs in about 5% of US women. [9] This can be a primary disorder, where the woman has never achieved orgasm or a secondary disorder, where the lack of orgasm results from another type of sexual dysfunction such as hypoactive sexual desire disorder or low sex drive. [9]
Another large nationwide survey found that about 5% of US women have a problem achieving orgasm and that causes them concern. [1] The survey found that the rate of problems with orgasm was higher among women ages 45 to 64 and those 65 or older (6% in both groups) than among women younger than 45 (3%).
Understanding Sex Pain
Learn More
Understanding Sex Pain
A significant number (17%- 45%) of perimenopausal and post menopausal women report experiencing pain during sex. This is called dyspareunia. The most common causes for this pain in women older than 50 are vaginal dryness and thinning of the vaginal tissues, both symptoms of a condition called vaginal atrophy. Another cause of pain during sex is vulvodynia, where women experience chronic pain in the vulva (the external part of female genitals).
Aside from the actual sensation of pain, anticipating or fearing pain during sex can cause anxiety and this in turn impacts sexual desire or the ability to become aroused. Concern about painful sex can also reduce lubrication and can cause vaginismus, which is involuntary, painful tightening of the vaginal muscles. [2]

Understanding Depression
Learn More
Understanding Depression
Approximately 40% of women experiencing any problems with sexual desire, arousal, orgasm, or pain are also experiencing depression. It is unclear if the depression triggers the sexual problems, or if the sexual problems trigger the depression. What is clear is that any woman experiencing sexual problems in the menopausal transition should also be screened for depression. [10]



0 in 2
postmenopausal women
never discussed their vaginal atrophy symptoms with a healthcare provider
If your vaginal dryness is caused by low estrogen levels, your healthcare provider may prescribe topical estrogen therapy. There are three methods of applying vaginal estrogen:
- Ring: You or your doctor can insert a soft, flexible ring into your vagina. It releases estrogen directly to the vaginal tissues. The ring lasts about three months so it will need to be replaced regularly.
- Tablets: These tablets are inserted into your vagina with a disposable applicator.
- Cream: The cream is inserted into your vagina using an applicator.
There are over-the-counter vaginal moisturizers as well. Speak to your pharmacist or your healthcare provider to get a recommendation. Water-soluble lubricants (such as Astroglide or K-Y Jelly) can also be used on an as-needed basis. Non-water-soluble lubricants, such as Vaseline, are not recommended if you are using condoms for either contraception or for prevention of STIs because they can weaken latex and reduce the effectiveness of the condom. [5]
During the menopausal transition, the state of the vagina often changes. Vaginal dryness and pain are symptoms of vaginal atrophy (atrophic vaginitis) that occur as a result of lowered estrogen levels. The tissues in the vagina weaken, get thinner, dryer, and may get inflamed, causing pain, burning, or discharge.
MYTH
While the changes happening to your body during the menopausal transition can impact a woman’s sexual health and sexuality, there are many treatment options available. Talk to your healthcare provider to see if you need any medical interventions such as a prescription for hormone therapy that can help with changes like vaginal dryness.
Oh yes they do!
A national study of 5,045 older women [11] showed the following:
| Sexual activity among older US women | |||||
| Age (years) | 50-59 | 60-69 | 70-79 | 80+ | |
| Masturbated in previous year | 54% | 46% | 36% | 20% | |
| Had intercourse (penis-vagina) in previous year | 51% | 42% | 27% | 8% | |
| Received oral sex in previous year | 34% | 25% | 9% | 4% | |
MYTH
While variable hormones during the menopausal transition can impact sexuality, there are many effective treatments that can restore sexual function. These include hormone therapy, vaginal lubricants, sexual aids, and counselling or therapy. Contrary to this myth, many women experience an increase in desire. This could be hormonal, but is also influenced by factors such as lowered stress and enjoying the privacy that comes when children move out of the house.
Compiled References
[1] Shifren JL, Monz BU, Russo PA, Segreti A, Johannes CB. Sexual problems and distress in United States women: prevalence and correlates. Obstet Gynecol. 2008 Nov;112(5):970-8. doi: 10.1097/AOG.0b013e3181898cdb. PMID: 18978095.
[2] https://www.menopause.org/for-women/sexual-health-menopause-online/sexual-problems-at-midlife
[3] https://www.webmd.com/menopause/guide/sex-menopause
[4] Lindau ST, Schumm LP, Laumann EO, Levinson W, O’Muircheartaigh CA, Waite LJ.
A study of sexuality and health among older adults in the United States. N Engl J Med
2007;357:762-774.
[5] https://www.webmd.com/women/guide/vaginal-dryness-causes-moisturizing-treatments
[6] Josefson D. (2000). FDA approves device for female sexual dysfunction. BMJ (Clinical research ed.), 320(7247), 1427.
[7] Billups KL. The role of mechanical devices in treating female sexual dysfunction and enhancing the female sexual response. World J Urol. 2002 Jun;20(2):137-41. doi: 10.1007/s00345-002-0269-0. Epub 2002 May 15. PMID: 12107545.
[8] Rosen RC, Shifren JL, Monz BU, Odom DM, Russo PA, Johannes CB. Correlates of sexually related personal distress in women with low sexual desire. J Sex Med. 2009 Jun;6(6):1549-1560. doi: 10.1111/j.1743-6109.2009.01252.x. Epub 2009 Mar 30. PMID: 19473457.
[9] Female Sexual Dysfunction: ACOG Practice Bulletin Summary, NUMBER 213. Obstetrics & Gynecology 134(1):p 203-205, July 2019. | DOI: 10.1097/AOG.0000000000003325
[10] Johannes CB, Clayton AH, Odom DM, Rosen RC, Russo PA, Shifren JL, Monz BU. Distressing sexual problems in United States women revisited: prevalence after accounting for depression. J Clin Psychiatry. 2009 Dec;70(12):1698-706. doi: 10.4088/JCP.09m05390gry. PMID: 20141709.
[11] Herbenick D, Reece M, Schick V, Sanders SA, Dodge B, Fortenberry JD. Sexual behavior in the United States: results from a national probability sample of men and women ages 14-94. J Sex Med. 2010 Oct;7 Suppl 5:255-65. doi: 10.1111/j.1743-6109.2010.02012.x. PMID: 21029383.
Not AI generated.
Original content, last updated February 22, 2023.
© 2024 Herstasis® Health Foundation