Monthly bleeding is a fundamental part of the menstrual cycle. The lining of the uterus thickens during your monthly cycle as it prepares to receive and nourish a fertilized egg. If no egg implants into the uterus, then the whole lining inside the uterus is shed through the vagina and out the vulva, resulting in a monthly flow of menstrual blood.
This process is completely driven by hormones, so it is not surprising that the variability in hormone levels during the menopausal transition impacts this monthly cycle and affects the regularity, heaviness, quality, and length of menstrual bleeding. Any of these issues, alone or in combination, can have a significant impact on a woman’s quality of life.


Perimenopause is the time when a woman transitions out of her reproductive years, ending in menopause when periods and ovulation have completely stopped for a full 12 months in a row. One of the hallmark symptoms of the menopausal transition is changes in the bleeding associated with your menstrual cycle. Commonly, the length and timing of the menstrual cycle become irregular, even to the point of getting a period every 2 weeks during perimenopause. Other changes include differences in the appearance and volume of menstrual blood. [1] If you experience vaginal bleeding after menopause (12 months without a period), or heavy bleeding after menopause that is bright red, see your healthcare practitioner immediately. Spotting after menopause is less concerning, although if it is frequent or becomes a flow, see your healthcare provider.
During the menopausal transition, your estrogen and progesterone levels are highly variable. These fluctuations vary from month to month and are often erratic, impacting ovulation and the rest of your menstrual cycle. This can be experienced as irregular or missed periods, as well as changes to your ‘typical’ menstrual bleeding.

Breakthrough Bleeding
Breakthrough Bleeding
Shedding small amounts of blood – too small to require the use of a tampon or a pad – is called breakthrough bleeding, or spotting. This happens when your changing hormone levels impact the buildup of the lining of your uterus, called your endometrium. Spotting is common just before or just after your period, but it also can happen mid-cycle. [2]

Heavy Bleeding
Heavy Bleeding
The lining of your uterus, called the endometrium, grows and thickens during your menstrual cycle in preparation for the implantation of a fertilized egg. Hormones are responsible for this, and as your hormones become variable during the menopausal transition, it can impact how much the uterine lining grows. As well, as your periods become more erratic and periods are skipped, the uterine lining will continue to thicken until it is shed during the next period. When the uterine lining is very thick, it can lead to heavy bleeding. Heavy menstrual bleeding is formally called menorrhagia.
Bleeding is considered to be heavy if you:
- soak through one tampon or pad every hour for several hours;
- need to use a tampon and a pad (double protection) to manage your menstrual flow;
- have to wake up to change your pad or tampon; or
- your period lasts longer than 7 days. [2]
Heavy bleeding can be very disruptive and affect your quality of life (QOL) as it can make it difficult or impossible to move normally through your day. Heavy bleeding can also cause fatigue and it increases your risk for iron deficiency anemia (IDA). [2][3] [4]

Changes in Blood Colour and Texture
Changes in Blood Colour and Texture
Women know what is typical during their own periods, so it can be concerning when the colour or texture of menstrual blood changes from the ‘norm’. Variation in colour or texture is normal. The colour of menstrual blood can range from bright red to dark brown. Darker colour blood is a sign that the blood leaving the body is older, which is nothing to worry about. The texture can also change from your normal flow, becoming thin and watery or thick and clot-like. [2]

Changes in the Length of Your Menstrual Cycle
Changes in the Length of Your Menstrual Cycle
As your estrogen levels decline, the lining of your uterus gets thinner. This can lead to lighter flow and menstrual cycles that are two or three days shorter than your normal cycle. In fact sometimes it can feel like you just finished your period and the next one is starting. This is common in the early menopausal transition. [1] [2]
As you move through the menopausal transition, however, your menstrual cycles may start to become longer and less frequent. A ‘long’ cycle is defined as any cycle that is longer than 38 days. This happens as you start to have more frequent cycles where you do not ovulate, or release an egg. These are called anovulatory cycles.
As you approach menopause, which is diagnosed as the absence of a menstrual cycle for 12 consecutive months, you may start to miss cycles completely. Be aware, though, that if you are still having periods, regardless of how infrequent they are, you are still ovulating. And that means you can still get pregnant. Unless pregnancy is your goal, ensure that you are still using birth control until you are fully in menopause, which indicates that your reproductive years are finished. [1] [2]
The irregularity of your periods can become frustrating but it will eventually end when you reach menopause.
Self-care & Natural Remedies for Bleeding Issues
Getting used to changing menstrual periods can be a challenge and can be frustrating.
There are a few things you can do to help manage your experience:

Record Your Cycles
Record Your Cycles
Record your cycles as this can help you visualize the patterns of your changing cycles. You can note any abnormal bleeding and discomfort, as well as any other symptoms you are experiencing. This is key information to share with your healthcare provider.
Evaluate the privacy & data protection policies for smartphone cycle-tracking apps before inputting any of your personal medical data, including cycle length.

Ibuprofen (Advil, Midol, Motrin)
Ibuprofen (Advil, Midol, Motrin)
Ibuprofen (Advil, Midol, Motrin) is used to help with the pain and cramping of your menstrual cramps, however it can also help reduce the flow of blood if you are experiencing heavy bleeding. Talk to your healthcare provider to find if this might work for you and if so, to find the best dosage for your individual needs. [2]

Protect Your Clothing
Panty Liners or Period Underwear
Leaks and stains are possible, so consider wearing thin pads or panty liners – many are disposable but there are reusable liners made of fabric if that is your preference.
Alternatively, invest in some black underwear or dedicated ‘period underwear’ so that you are not staining all of your undergarments.

Use Birth Control
Continue to Use Birth Control
Remember to use birth control! As long as you are getting periods, no matter how infrequent, you are ovulating and this means you can get pregnant. Unless pregnancy is something you want, be sure to use reliable birth control. [2]
Therapy & Treatment for Bleeding Issues
At age 40 find a reliable, educated primary care provider familiar with recognizing and treating symptoms of perimenopause and menopause. The North American Menopause Society provides a list of menopause practitioners here.
Bleeding issues such as changes in length of flow, heaviness of flow, and changes in colour and texture of blood are almost certain to happen as you move through the menopause transition towards menopause. Despite this, changes in your usual bleeding patterns can be a sign of other, more serious, problems such as abnormal growths inside your uterus (called endometrial hyperplasia). [1]

See your healthcare provider if you have:
- ▢ Any concerns about your bleeding
▢ Extremely heavy bleeding (when you need to change your pad or tampon every hour)
▢ Bleeding that goes on for more than seven days
▢ Bleeding (not spotting, but rather a menstrual flow) that happens more frequently than every 3 weeks
▢ Menstrual flow that contains blood clots larger than the size of a quarter.
This heavy bleeding is called menorrhagia. You will likely have a pelvic exam, blood tests, and possibly an ultrasound, all of which are used to rule out serious problems. [2]
Getting a proper diagnosis requires ruling out other possible reasons for your heavy bleeding. Blood tests will check for anemia and blood clotting factors, a pap test will rule out cancerous growths, infection or inflammation, and an ultrasound may be used to check for fibroids in the uterus. Based on the results from those tests, you may get a biopsy, which is a tissue sample from the uterine lining or a hysteroscopy, which uses a small camera inserted through the vagina to directly examine the cervix and the inside of the uterus. Finally, you may require a procedure known as a dilation and curettage (D&C), where the lining of the uterus is scraped away so the inside of the uterus can be examined. [2] [5]
- Oral contraceptives are a common medical treatment for very heavy periods, however, they may not be effective to treat menorrhagia.
- Prostaglandin inhibitors are nonsteroidal anti-inflammatory drugs, including aspirin or ibuprofen. They may be helpful in reducing the amount you bleed and can also be helpful for cramping.
- An Intrauterine Device (IUD) that releases progestin in has been shown to be a more effective therapy, and can be prescribed to treat heavy bleeding for up to five (5) years. [2][6]
If these approaches do not help your heavy bleeding, other medical treatments to explore with your Doctor healthcare provider include endometrial ablation (surgical removal of the uterine lining), a hysterectomy, and/ or surgical removal of any fibroids or cysts in the uterus or ovaries. [2] [5]
The Science
Among women in the early menopause transition, abnormalities in timing of menstrual bleeding – both changes in the length of your cycle or changes in the number of days you typically bleed – are the result of changes in hormone levels. These changing hormones also result in anovulation, cycles where you do not ovulate, or release an egg.
Abnormally heavy periods, however, do not appear to require hormonal fluctuations. In some studies, heavy periods are more closely associated with obesity (a body mass index (BMI) of 30 and above) and the presence of benign fibroids (leiomyomata). [2] Heavy periods can be identified by:
- needing to change your pad or tampon every hour;
- bleeding that goes on for more than seven days;
- bleeding (not spotting, but proper menstrual flow) happens more frequently than every 3 weeks; and/or
- have a menstrual flow that contains blood clots larger than the size of a quarter.
Heavy periods are less likely after anovulatory cycles where no egg was released. [2]

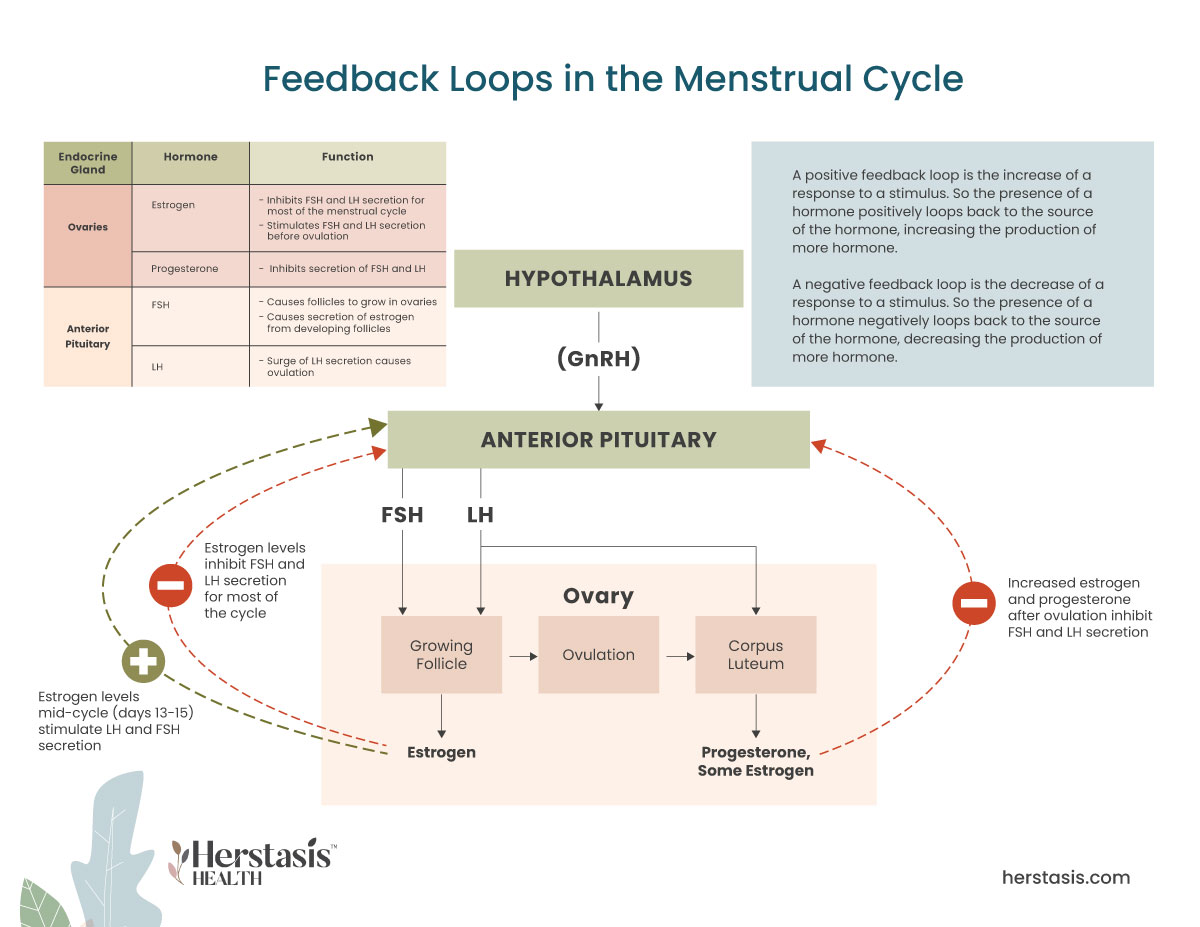
The different hormonal and physical processes driving your menstrual cycle. [5]
The menstrual cycle involves the monthly release of an egg from one of the ovaries, a process called ovulation. The uterus prepares to receive a fertilized egg via a series of hormonal changes. If the egg does not get fertilized by a sperm cell then the lining of the uterus isn’t needed and it is shed through the vagina – resulting in a menstrual period. [4]
This menstrual cycle is driven by changes in hormones, particularly estrogen, progesterone, luteinizing hormone (LH) and follicle-stimulating hormone (FSH). Estrogen and progesterone are called ‘sex hormones’ because they are secreted by your ovaries, which are the female sex organs. LH and FSH are gonadotropins because they are secreted from cells in the anterior pituitary called gonadotrophs (gonads are the formal term for the sex organs – ovaries in females, and testes in males).
There are three stages in the menstrual cycle: the follicular stage (before release of the egg); the ovulatory stage (egg release); and the luteal stage (after egg release).
The first day of menstrual bleeding marks the first day of the follicular phase. At this time, levels of estrogen and progesterone are low and the top layers of the thickened lining of the uterus (endometrium) break down and shed, creating the menstrual bleeding. At the same time, follicle-stimulating hormone (FSH) levels increase and cause several follicles, each containing an egg, to develop in the ovaries. Then the FSH levels start to decrease and only one follicle continues to develop and starts to produce estrogen.
This becomes the ovulatory phase when luteinizing hormone (LH) and FSH both rapidly increase. LH causes the egg to be released from the follicle (ovulation). Estrogen levels decrease when LH and FSH levels are heightened. Progesterone levels begin to increase.
In the luteal phase both LH and FSH levels decrease. A structure called the corpus luteum forms from the ruptured follicle (that just released the egg) and it begins to produce progesterone. Estrogen levels stay elevated for much of the luteal phase. The presence of progesterone and estrogen cause the uterine lining to thicken in preparation for the implantation of a fertilized egg.
If the egg isn’t fertilized, the corpus luteum breaks down and stops producing progesterone. Estrogen levels also decrease. This causes the top layers of the uterine lining to break down and begin shedding, starting menstrual bleeding and the beginning of a new menstrual cycle. [4] [5]
Myths & Mysteries
When you have not had a period for one full year (12 months), you have officially entered menopause.
The most common reason for spotting after menopause is hormonal imbalance. This can be caused by a variety of factors, including changes in diet, stress levels, and medications. Other potential causes of spotting after menopause include uterine fibroids, endometriosis, and ovarian cysts. In rare cases, spotting after menopause may be a sign of cervical or endometrial cancer.
During perimenopause, the time before the period ceases, it is normal for women to experience bleeding that is heavier than usual. This bleeding can last for a few days to a few weeks. In some cases, the bleeding may be so heavy that it interferes with a woman’s daily activities. If this occurs, it is important to see a doctor to determine the cause of the heavy bleeding.
The answer to this question is not entirely clear. There is some evidence that heavy bleeding may occur before menopause, but the research on this topic is still relatively limited. It’s possible that heavy bleeding may be a symptom of perimenopause, which is the transition period leading up to menopause. During perimenopause, hormone levels fluctuate and can cause changes in the menstrual cycle, including longer or shorter periods, or heavier or lighter bleeding.
The most common reason for spotting after menopause is hormonal imbalance. This can be caused by a variety of factors, including changes in diet, stress levels, and medications. Other potential causes of spotting after menopause include uterine fibroids, endometriosis, and ovarian cysts. In rare cases, spotting after menopause may be a sign of cervical or endometrial cancer.
NOPE, not true at all.
The blood that leaves your body during menstruation isn’t toxic, and it isn’t ‘bad’ in any way. Rather it is a normal, healthy result of your menstrual cycle. Menstrual blood will not interfere with your sexuality and it does not mean you are unclean in any way.
FALSE
Birth control pills are often used to manage menstrual blood flow and are commonly prescribed for heavy bleeding. Older versions of birth control pills did have high doses of estrogen, which increased the risk of blood clots in women over 35, however today’s birth control pills use much lower doses of estrogen and do not carry the same risks. In fact, today’s birth control pills are known to have benefits that include a lower risk of ovarian and endometrial cancer. Birth control pills are not recommended for women over 35 who smoke, have high blood pressure, or have a history of heart disease.
YES
There are several treatment options available, some of which, like a hormonal IUD, can be used to treat heavy periods for up to five years. Talk to your healthcare provider to find the best solution for you.
YES
Heavy bleeding and/or long menstrual periods can lead to health issues including iron deficiency anemia (IDA). As well, heavy bleeding can have a major negative impact on a woman’s quality of life because it can interfere with daily activities.
NO
Not true. Heavy bleeding during the menopausal transition is linked to obesity and fibroid tumours. If you experience heavy bleeding and are not in the menopausal transition, talk to your healthcare provider to rule out any serious health issues.
FALSE
Heavy periods that involve losing more than 80mL of blood (5.5 tablespoons) are not normal. This condition is called menorrhagia and current research suggests they are not totally hormonally driven. Rather they are also linked to obesity and/or the presence of fibroids (fibroid tumours). [5]
Citations
[1] Van Voorhis BJ, Santoro N, Harlow S, Crawford SL, Randolph J. The relationship of bleeding patterns to daily reproductive hormones in women approaching menopause. Obstet Gynecol. 2008 Jul;112(1):101-8. doi: 10.1097/AOG.0b013e31817d452b. PMID: 18591314; PMCID: PMC2666050.
[2]https://www.healthline.com/health/menopause/perimenopause-periods
[3] https://www.webmd.com/women/news/20130104/iud-heavy-menstrual-bleeding
[4] Anne Firquet,Wolf Kirschner &Johannes Bitzer. Forty to fifty-five-year-old women and iron deficiency: clinical considerations and quality of life. Gynecological Endocrinology. 2017; 33 (17):503-509
[5] https://www.hopkinsmedicine.org/health/conditions-and-diseases/menorrhagia
[6] Gupta J., Kai J., Middleton L.; Pattison H., Gray R., and J. Daniels Levonorgestrel intrauterine system versus medical therapy for menorrhagia. N Engl J Med. 2013; 368: 128-137
Not AI generated.
Original content, last updated May 30, 2024.
© 2024 Herstasis® Health Foundation