What is the Male Mid-life Crisis?
What is Male Menopause?
What is Andropause?
Male Mid-life Symptoms
Erectile Dysfunction
Loss of Libido
Support Your Partner
Therapy & Treatments
Self-care & Natural Remedies
Science
Myths and Mysteries
What is Male Menopause – Manopause?
Manopause. Male menopause. Midlife crisis. Andropause.
These terms are used interchangeably in the marketplace, and are confusing because men do not have the same drastic fluctuations and changes in sex hormones that underlie the female menopause.
Yet, so many men aged 40-60 experience such significant emotional and physical changes that we do need a name for this stage of life. This will allow men to start to talk openly with their family and employers about their challenges, and seek medical help when appropriate.
Whereas andropause is a true medical condition, often caused by injury, disease or medication, and there is overlap between the symptoms of andropause and midlife, we will use the terms “male midlife” and “male midlife crisis” to recognize the significance of the male experience of aging without confusing it with hormone change.
What is the Male Mid-Life Crisis?
A mid-life crisis is a relatively common experience in men, and it can be an extremely chaotic and tumultuous time. A ‘typical’ midlife crisis is defined as a period or phase of life, usually between the ages of 40 and 60, when a man begins to question their accomplishments or achievements in their lives to date. While ‘crisis’ is the common term used for this experience, in fact it is a natural process that can, in the best case scenario, include re-assessment, adjustment and acceptance. A midlife crisis can also be a factor contributing to male menopause, which is discussed here. [7] [7c]
Signs you may be experiencing a mid-life crisis as you turn 40 or older include:
General Dissatisfaction
Experiencing general dissatisfaction with life, or questioning your existing life choices

Downhill From Here
A sense that your best days are behind you, that it’s all ‘downhill’ from here

Trapped
Feeling trapped in your life
No Time
Experiencing a sense of running out of time to make any life changes or life decisions
Mood Swings
Increasing mood swings or mood changes

Increased Anger
Increasing anger at the world in general for being unfair
Targeted Anger
Increasing anger at specific individuals (such as bosses or family members) that you perceive to have held you back or been unsupportive

Withdrawing
Withdrawing from work, family, and life in general [7] [7a]

Destructive Behaviour
Exhibiting changes in behaviour, especially destructive ones that are listed below…
Destructive Behaviors
- starting or increasing drinking and illicit drug use
- starting or wanting to start an extra-marital affair
- spending money on atypical items (like a sports car or a new boat)
- spending money recklessly and/or beyond your means
- leaving or wanting to leave your family
- taking up high-risk sports and hobbies like sky-diving or rock climbing
- having more focus on and changing your appearance, by changing the way you dress, significantly increasing your workouts, or considering (or having) cosmetic surgery
- dropping long-time friends and relationships
When will my Mid-life Crisis Go Away?
It is possible to come out of your mid-life crisis better and happier than when you went into it because a mid-life crisis leads to either ‘growth or destruction’. The growth happens when men consider the underlying causes of unhappiness and dissatisfaction, and make careful and thoughtful decisions and plans to change and address those causes.

Unfortunately, you may come out of your mid-life crisis much less happy and satisfied than when you went in if you follow the destruction path. This happens when poor choices and insufficient positive actions result in radical changes such as leaving your family or spending money beyond your means.

These destructive choices may feel like they are going to improve your life and your circumstances in the moment, but instead they often destabilize your life and remove carefully built community support systems. [7b] [7c]
What Are Male Mid-life Symptoms?
Men experience real and sometimes debilitating physical and mental midlife symptoms, although they may not always report these to their healthcare provider immediately. These symptoms overlap with andropause symptoms and male menopause symptoms and often interfere with day-to-day life. They can impact not just the men experiencing them, but also their friends, family and co-workers.
The most common symptoms include:
- depression
- loss of sex drive
- erectile dysfunction
- mood swings and irritability
- anger
- loss of muscle mass and reduced ability to exercise
- fat redistribution, such as developing a large belly or “man boobs” (gynaecomastia)
- a general lack of enthusiasm or energy
- difficulty sleeping an/or or increased tiredness
- night sweats
- hot flashes
- poor concentration and short-term memory challenges

What are Andropause and Late Onset Hypogonadism (LOH)?
Testosterone – the main male sex hormone – goes through a slow, steady and progressive drop at a rate of about 1% per year starting in men’s 30s and 40s. This is not a medical condition, rather it is a normal and natural part of aging. The rate of decline in testosterone levels varies in different individuals and it can be affected by chronic disease, excess weight, illness, serious emotional stress, and medication side-effects. This natural rate of testosterone decline can be slowed (but not stopped) by making changes to lifestyle and behaviours.
There are medical diagnoses resulting from low testosterone levels. Andropause is a medical condition that exists when there are no or extremely low testosterone levels. True andropause exists only in men who have no functioning testicles, due to illness, disease or accident. This can happen at any time of life – some men are born with andropause – so andropause is not specific to mid-life, although it may be diagnosed at that time if the testes stop functioning due to an illness or injury that happens mid-life.
Testosterone deficiency that develops after midlife is diagnosed by endocrinologists and is known as late onset hypogonadism (LOH). LOH may be responsible for some male midlife symptoms, but many symptoms are not associated with hormones at all. [1] [2] [3] [4]
It is common to use the term andropause to describe changes many men experience starting in their late 40s and 50s, including sexual symptoms like loss of libido, erectile dysfunction, loss of muscle mass, depression and mood swings. This is incorrect unless the testes stop functioning during a man’s mid-life.
The media often use the term ‘manopause’ and male menopause interchangeably with andropause. This is incorrect. These conditions are different – the underlying cause of andropause is a diagnosable medical condition of low or no testosterone whereas male menopause does not have a hormonal basis comparable to female menopause. And to add more complexity, LOH, not andropause, is the proper term for testosterone deficiency starting at or after mid-life that may cause the symptoms experienced in men.
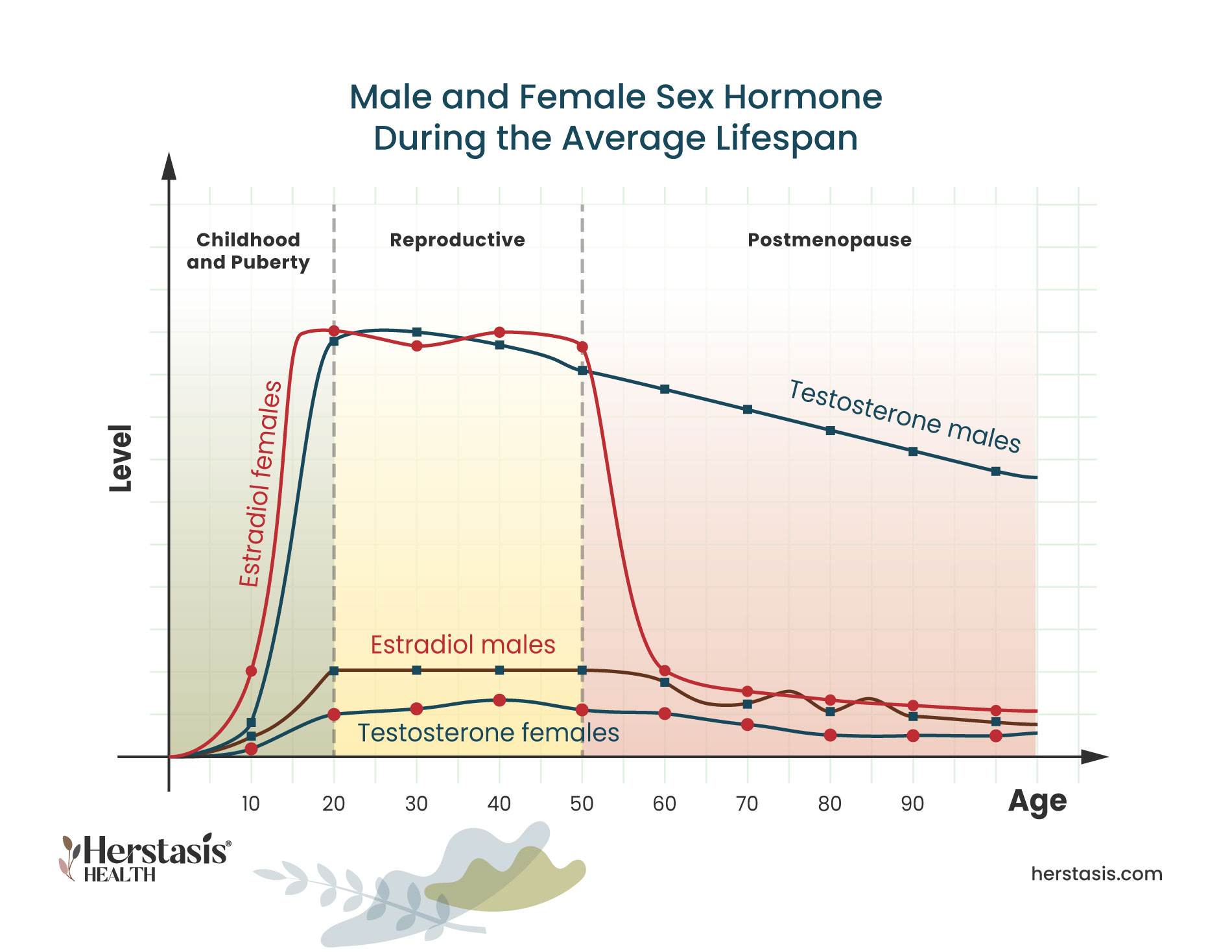
It is easy to think that male and female menopause must have a similar underlying hormonal basis, however, this isn’t true. In females, estrogen – the main female sex hormone – begins an abrupt decline after a woman’s reproductive years, followed by years of variability before finally settling into steady but low levels that will persist throughout their lives.
In contrast, testosterone – the main male sex hormone – goes through a slow, steady and progressive drop at a rate of about 1% per year starting in men’s 30s and 40s. This is not the medical condition of either andropause or LOH. Instead the decline is a normal and natural part of aging. The rate of decline in testosterone levels varies in different individuals and it can be affected by chronic disease, excess weight, illness, serious emotional stress, and medication side-effects. This natural rate of testosterone decline can be slowed (but not stopped) by making changes to lifestyle and behaviours. [1][2][3][4]

What is Erectile Dysfunction?
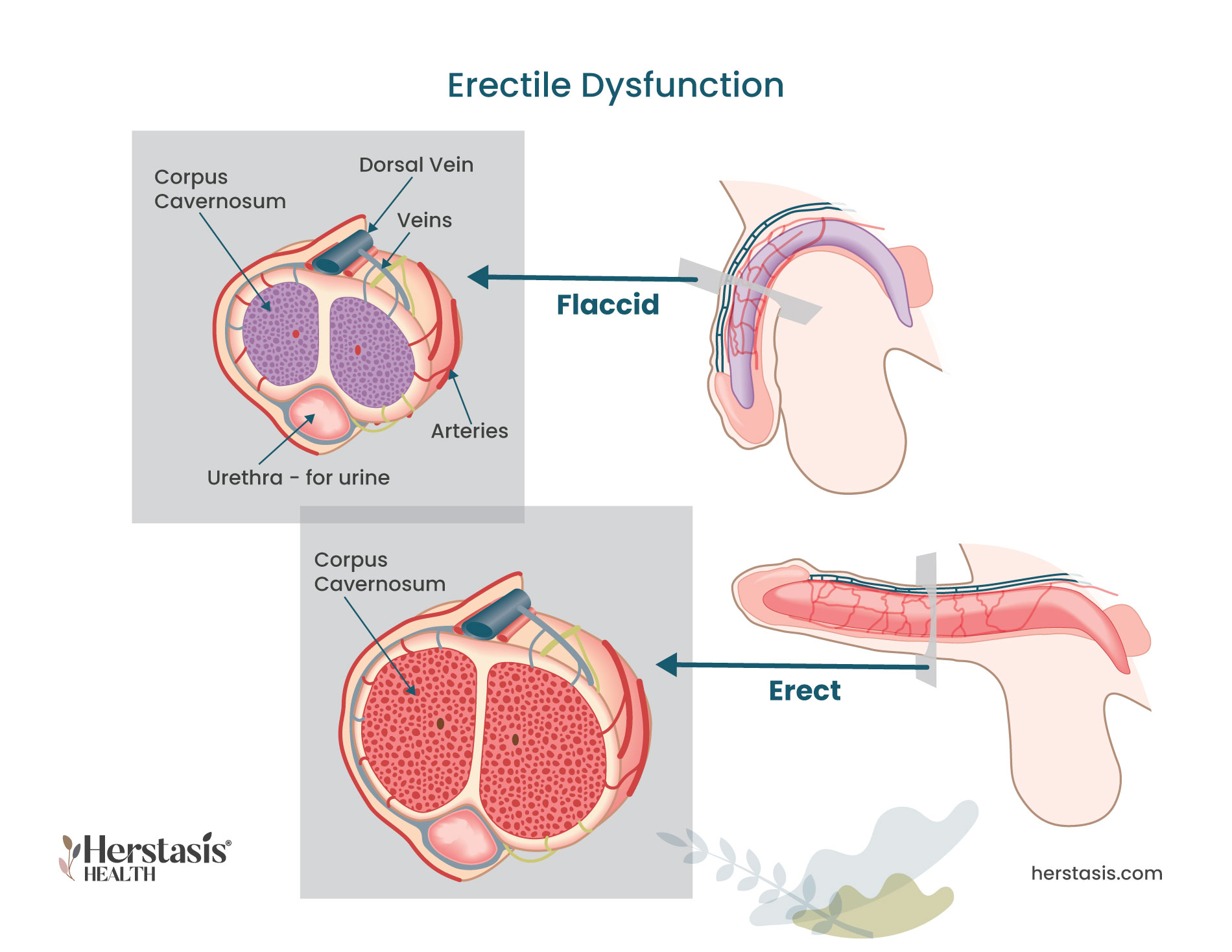
Experiencing difficulty achieving and maintaining an erection sufficient to participate in sexual activity can be very hard to accept but there are ways to manage and overcome this symptom. Many men don’t seek or delay getting help because they are embarrassed. Don’t be! Ongoing ED severe enough to be reported to a physician affects over 30 million men in the US alone.
Erectile dysfunction (ED) does happen to almost every man at some point in their lives. The penis contains two sponge-like structures called the corpora cavernosa. These are basically two cylinders that extend the length of the penis. Sexual arousal causes increased blood flow to both of these cylinders and the influx of blood causes an erection by expanding, straightening, and stiffening the penis. [13]
The causes of ED can be physical or they can stem from emotional and psychological issues.
The physical causes of ED include:
- Not enough blood flow to the penis. This can happen for a number of reasons including heart and cardiovascular disease, diabetes (which can cause small blood vessel and/or nerve damage), and smoking.
- The penis cannot hold available blood. If blood doesn’t stay in the penis, erection isn’t possible.
- Nerve signals from the brain or spinal cord do not reach the penis. This can happen as a result of some diseases, injuries, or nerve damage in the pelvic region.
- Surgery and or radiation for cancers in the lower abdomen or pelvis. ED is a common side effect of prostate, colon-rectal or bladder cancer treatments.
- Other medications used to treat other health problems.
Emotional and psychological causes of ED include:
- depression
- anxiety
- relationship problems
- stress
- lack of self-confidence about sexual performance.
If you have a partner going through the menopause transition who has a diminished interest in sex, feelings of inadequacy and frustration can take over, causing issues for your own sexuality. Women taking medications for depression or anxiety may also experience a loss of libido or inability to orgasm which can be frustrating for both of you.
What can I do about ED?
Knowing the likely cause(s) of ED is the key to resolving it with the correct therapy. Physical treatments will use medications – either new ones or adjusting and changing your existing ones. You may also need to make lifestyle changes that include improving your nutrition, getting adequate sleep, and increasing your movement and activity levels.
In some cases, men may be prescribed a vacuum constriction device (VCD), also known as a penis pump. This device is an external cylindrical pump that is placed over the penis. Air is pumped out of the cylinder it creates a vacuum, and this vacuum draws blood into the shaft of the penis. The blood will cause the penis to swell and become erect. Once the erection is achieved, a retaining band is placed at the base of the penis to hold the blood in. The pump is removed and the band can safely stay in place for up to 30 minutes, allowing for intercourse. Use of the VCD will cause an erection, but there are differences when compared to a natural erection. Side effects from using the pump include a purplish colour to the penis, numbness, bruising and swelling of the penis and difficulty achieving orgasm. Additionally, ejaculation is unlikely and the penis will be cold. Warm compresses can be used to increase the penis temperature before intercourse. [14]
If the causes of your ED are emotional or psychological, counselling, talk therapy, meditation, and/or breathing exercises can help. The vacuum constriction device discussed earlier in this section is safe and has few long-term side effects. Because of this, it may be prescribed for use when the cause of ED is psychological. This is not a permanent solution, but will allow for successful intercourse while other treatments such as counselling, are ongoing. Talk to your healthcare provider to find a solution that works for you. [13 [14] [15]

Decreased Libido (Decreased Sex Drive)
A decrease in your libido means you have a lowered sex drive, reducing your desire to have sex. You will have less frequent sexual thoughts and fantasies and you may engage in sexual activity less frequently. When libido is low, sexual stimulation can fail to cause interest.
Libido is not usually associated with the ability to achieve an erection, so men with a low libido can still engage in sexual activity to satisfy their partner. Having to do this, however, may impact your overall relationship with your partner and can also have significant psychological effects for you. [16]
There is no ‘typical’ level of libido, and sex drive varies among men. As men age, there is a tendency to see a gradual decrease in libido, but age-related changes are gradual, if at all. Fatigue, anxiety, stress, or other conditions may cause temporary reductions in libido and this is normal throughout a man’s life. When noticeable changes to your libido develop after years of ‘normal’ levels of sexual desire, this can be very disruptive to relationships, and can also affect your self-esteem.
Psychological factors, such as long lasting depression, anxiety, alcoholism, illicit drug use, chronic fatigue, and/or relationship stress are often the root cause of low libido. Physical factors such as chronic kidney disease can decrease libido, as can some drugs, including those used to treat depression, anxiety, or advanced prostate cancer. These types of drugs may decrease blood levels of testosterone resulting in a lower libido. [16] [17]
What can I do about my low libido?
Treatment for low libido depends on the root cause. Treatments for psychological and emotional issues include talk therapy as described in a different section of this page, as well as practices described in the Self-care section. These include practicing meditation and/or breathing exercise, journaling your thoughts and feelings, joining a support group or a peer group and/or practicing Mind Body Wellness therapies. Refer to the Herstasis therapy page Mind Body Wellness to explore options for alternative and complementary treatments that may help you. Yoga, biofeedback and relaxation therapy, hypnosis, aromatherapy, meditative movement such as Tai Chi or Qigong, are all described in detail, as are several others. You may get inspired to try one or more of these and see if it helps any of your symptoms. [1]
A blood test can measure the level of testosterone in the blood. If this is the root cause of a low libido, it can be treated with testosterone replacement therapy (TRT) as described in a separate section.
Causes of Male Mid-Life Symptoms
It can be difficult to pin down the exact reasons for men’s mid-life symptoms. Low testosterone is often blamed, but it is rarely the primary cause unless there is a clear illness or injury to explain lowered hormone levels. Given this, it is important to recognize that lifestyle choices can be a factor, as well as psychological issues. For example, erectile dysfunction can result from stress, depression, and/or anxiety, but it is also associated with obesity, smoking, excessive drinking, and cardiovascular health problems. [1]
Common causes of male menopause symptoms include:
- stress
- anxiety
- lack of sleep
- a poor diet
- lack of exercise
- drinking too much alcohol
- smoking
- low self-esteem [1]
Night sweats in men can be caused by low testosterone, but more commonly results from anxiety and/or stress, diet, alcohol, medications, or a side effect of sleep apnea. This is true of hot flashes during the day in men as well, where the most common causes are anxiety, stress, or side effects of medication. [5][6]
Self-care and Natural Remedies for Symptoms of Male Mid-life Crisis, Male Menopause, and Andropause
It is important to understand the root causes for any symptoms you may be feeling. Know that midlife is often a time of self-reflection and self-assessment, both of which can play an important role in symptoms experienced for midlife men. Self-care for your symptoms can play an important role in helping reduce their impact, regardless of the causes.

Talk to someone you trust. Sometimes just sharing your experiences provides some perspective and can lower your anxiety or stress.
Take care of your physical body. When you eat well, get adequate exercise, and have good quality sleep, you will feel better. Full stop.
Exercise with friends. Make connections with people while you are doing something good for your body and make it a regular thing you look forward to.
Practice meditation and/or breathing exercises. Daily practices like “box breathing” help calm your mind and give you a smart tool for reducing the strength of mood swings, anger, depression or other behavioural symptoms in the moment they happen.
Journal your thoughts and feelings. Not only is keeping a journal a proven way to self-reflect and practice self-care, your journal can also help you track your symptoms. You may start to see patterns and identify situations that trigger scary and uncharacteristic feelings and behaviours. Take the time to journal things that are good as well! This can be a boost when you are feeling down or irritated.
Join a support group or a peer group. Your healthcare provider can give you a recommendation for a support group or point you to specialty care organizations that provide support for midlife men.
Practice Mind Body Wellness therapies. Refer to the Herstasis therapy page Mind Body Wellness to explore options for alternative and complementary treatments that may help you. Yoga, biofeedback and relaxation therapy, hypnosis, aromatherapy, meditative movement such as Tai Chi or Qigong, are all described in detail, as are several others. You may get inspired to try one or more of these and see if it helps any of your symptoms. [1]
Therapies and Treatments for Symptoms of Male Mid-life Crisis and Male Menopause
If you’re experiencing symptoms that could be caused by male menopause, see your healthcare provider. You will get tested for hormone levels, and you can also expect to discuss your work and personal life to see if your symptoms may be caused by problems such as stress, anxiety, poor sleep, or excess weight.

What are talk therapies?
If stress or anxiety are affecting you, you may benefit from some form of professional talk therapy, also called psychotherapy. One useful type of talk therapy is cognitive behavioural therapy (CBT). This type of psychotherapy is based on the idea that your thought patterns affect your emotions, which can then affect your behaviors.
CBT can teach people different ways of thinking, behaving, and reacting to situations to help reduce anger, anxiety or depression. For example, CBT recognizes that negative, worrying thoughts can lead to fearful, worrisome feelings and actions. Purposefully reframing your thoughts to be more positive can lead to more positive feelings and helpful behaviors. [1]
With a therapist using CBT, you will:
- identify specific problems or issues in your daily life
- increase your awareness of negative thought patterns and how they can impact your life
- identify negative thinking and reframe it in a way that changes how you feel
- learn new behaviors and put them into practice [8]
Exposure therapy is a technique used in CBT that has patients confront the fears underlying their anxiety. This helps get individuals back doing activities that they have been avoiding due to anxiety. Relaxation techniques are used to help manage anxiety while doing the exposure therapy. [9]
Acceptance and commitment therapy (ACT) is another type of therapy that can be used specifically to treat anxiety. ACT teaches strategies such as mindfulness to reduce anxiety. It is a newer form of therapy than CBT, so at this time, less information is available on its long-term effectiveness. [9]
Anger Management Therapy
Anger is a common response to feelings of threat, stress, helplessness, or frustration. It is a totally normal emotion, just like fear or happiness. Everybody experiences anger at some point in their lives. Feelings of anger can trigger the release of cortisol and/or adrenaline, both of which are hormones that work together in the fight, flight, or freeze response that is an adaptive response that helps get us out of difficult or dangerous situations. Anger is also a normal way to deal with negative feelings and can motivate us to find solutions to the problems that are causing the anger.
Repeated bouts of anger on its own, with no appropriate trigger, is not normal. Unfortunately, anger outbursts are a common symptom during male midlife. Managing anger is possible and help is available if anger is affecting relationships and other important parts of your life. Common anger management therapies and techniques are often blended into different types of talk therapies.
These therapies and techniques include:
- Joining a support group for anger management. This will help you understand your anger including your key triggers. Group support is very useful to develop strategies and skills that will help you manage anger and any other difficult emotions that may be appearing with no apparent cause.
- Individual counselling. There are various techniques and tools that can be used to help manage anger. Cognitive behavioural therapy (CBT), discussed in the Talk Therapies section is a common approach that typically shows successful results.
- Cognitive restructuring. This is an element of several types of talk therapies, and it can also be applied on its own. Cognitive restructuring involves adjusting unhelpful, inflammatory thoughts and beliefs by identifying and challenging them. It can also be applied to other parts of daily life to help manage stress, improve relationships and improve professional behaviours.
- Identifying triggers. This therapy helps you to detect what things, people, and/or events set off an anger outburst. Once triggers are identified, anger management therapy will help you develop alternative healthy responses.
- Deep breathing techniques, visualization techniques, and/or meditation can be used to slow down your heart and breath rates and calm your nervous system. This is an excellent practice that can be used ‘in the moment’, and it helps ‘take down the temperature’.
- Progressive muscle relaxation is often part of a meditation or visualization technique that helps to release tension, change your focus away from your anger, and calm your nervous system.
- Emotion labeling. Learning to identify and label your emotions is a big step towards controlling them. [10] [11] [12]
Anger can be a very destructive emotion, causing distress and damage to yourself and others. When you are ready to seek counselling specifically to manage your anger, make sure you find a qualified therapist. There are many different therapists out there, and doing some homework will ensure that you get a good match between your therapist and your needs.
Ask (and get satisfactory answers) to the following questions:
- What are their qualifications?
- Are they certified and regulated by a professional body?
- What is their specialization, if they have one?
- How long have they been practicing, and is all of that experience in anger management?
- What techniques do they use most commonly?
- Do they have any positive reviews from past clients?
- How do they define success, and what is their success rate? [12]
There is no shame in seeking help. If this is a new approach for you, trust in the process. Seeking help is a huge step towards resolving your anger, repairing any damage you may have caused in your life, and finding peace during this challenging time of life.
Testosterone Replacement Therapy
If testosterone levels are low (hypogonadism) there are benefits from testosterone replacement therapy (TRT). Testosterone replacement therapy is available in oral, transdermal, transbuccal, intramuscular, and subcutaneous implant forms. [18] In some cases, testosterone may be self-injected, however this is only safe when prescribed by a physician and with proper and sufficient training.
Any use of testosterone without a prescription can be dangerous as there are many side-effects, including more aggressive and irritable behaviour, more acne, increased skin oils and causing or worsening of sleep apnea.
Studies have revealed a clear association between low testosterone levels and changes in sexual function, body composition (body fat distribution), physical functioning and mobility, and increased risk of diabetes, late life persistent depressive disorder (dysthymia), unexplained anemia of aging, osteoporosis and bone fractures. However, it is important to distinguish between low testosterone from illness or injury (true hypogonadism) and declining levels of testosterone because of increasing age.
Testosterone has been shown to clearly benefit younger men with hypogonadism. However, the use of testosterone replacement therapy in aging men is controversial, as neither the long-term benefits of improved health outcomes nor the long-term risks of testosterone therapy are known. [18] [19] Further studies are underway to determine if testosterone therapy might stimulate growth of metastatic prostate and breast cancer. Testosterone therapy may also increase the risk of heart attack and stroke and contribute to the formation of blood clots in the veins. [20]

Anxiety Medications
Learn More
Anxiety Medications
There are medications that work specifically to reduce the symptoms of anxiety including panic attacks and extreme worry and fear. Benzodiazepines are the most common class of anti-anxiety medications. They are very effective in helping to reduce anxiety, and they start working more quickly than most antidepressant medications. Benzodiazepines are the first-line treatment for generalized anxiety disorder.
Unfortunately, it is easy to build up tolerance to benzodiazepines and start requiring higher and higher dosages to get the same calming effect. It is possible to become dependent on them and to experience withdrawal symptoms when the medication is stopped. Because of this, your health care provider will probably only prescribe benzodiazepines for a short period of time. If you are on benzodiazepines, your healthcare provider can work with you to safely decrease your dosages when you are ready to stop using them. [9]
Antidepressants are helpful to treat anxiety as well as depression. Anxiety is closely linked to the neurotransmitter molecule serotonin. Taking Selective Serotonin Reuptake Inhibitors (SSRIs) can help anxiety by working to maintain high circulating levels of serotonin in the blood. The Science section provides more detail on serotonin, and how it works to help in the treatment of anxiety. [9]
Beta-blockers are a medication usually used to treat high blood pressure. They are very useful to help relieve the physical symptoms of anxiety, including rapid heartbeat and shaking or trembling. They can also be used on an as-needed basis to help with episodes of acute anxiety, including some predictable forms of social anxiety such as public speaking or performing. [9]
The Science
Hypogonadism and Late Onset Hypogonadism (LOH)
Hypogonadism occurs when the testes produce few or no hormones. It can be present from birth, which can cause symptoms like delayed puberty and small testes. Hypogonadism can also occasionally develop later in life, known as late-onset hypogonadism (LOH), and it is most common in men who are obese or have type 2 diabetes. When this occurs, it can cause male menopause symptoms. It is important to realize though, that LOH is not a normal part of aging, rather it is a specific medical condition. A diagnosis of late-onset hypogonadism can usually be made based on the presence of symptoms plus the results of blood tests used to measure your testosterone levels. [1]
The most common symptom of testosterone deficiency is low libido, and other common symptoms include erectile dysfunction, decreased muscle mass and strength, increased body fat, decreased bone mineral density and osteoporosis, and depression. None of these symptoms alone are specific only to low testosterone, but if any of these are present, ruling out low testosterone is the first step. It is important to exclude other common causes of these symptoms, including depression, hypothyroidism, chronic alcoholism, and use of medications such as corticosteroids, cimetidine, spironolactone, digoxin, opioid analgesics, antidepressants, and antifungal agents before making a diagnosis of LOH. [2]
Testosterone is measured in units of nanomoles (nmoles) per litre (L). A mole is an amount of a substance that contains a very large number (6 followed by 23 zeros) of molecules or atoms. A nanomole is one-billionth of a mole. A litre measures fluid volume. Testosterone can also be measured in nanograms (ng) per deciliter (dL). A nanogram is one-billionth of a gram (which is about 1/30 of an ounce) and a decilitre measures fluid volume that is 1/10 of a litre.
Testosterone can be found circulating in the body in ‘free’ form, where it is on its own, or it can be circulating in a form where it is ‘bound’ to proteins. About 98% of the body’s testosterone is bound to either SHBG (sex-hormone binding globulin), or to the protein albumin. Only 2% of the body’s testosterone is found in free form. Total testosterone, also called total serum testosterone, measures all testosterone in the blood, both free and bound forms. Free testosterone levels are significantly correlated with libido, erectile, and orgasmic function.
There is general agreement amongst various professional bodies that total testosterone levels above 12 nmol/L (350 ng/dl) does not require testosterone supplementation. There is also a consensus that patients with total testosterone levels below 8 nmol/l (230 ng/dl) will usually benefit from testosterone treatment. If the total testosterone level is between 8 and 12 nmol/l (230 and 350 ng/dl) the tests can be repeated to look only for free testosterone. This measure will help determine whether or not the individual needs additional testosterone added to their system. [2]
Myths & Mysteries
The roots of most male male menopause symptoms are usually related to lifestyle and behaviour problems. The first step for men experiencing symptoms in midlife is to check their testosterone levels in case that is a factor. But typically lifestyle changes such as improving diet, sleep, and exercise habits as well as treatment for any anxiety, stress or depression will help manage or even correct the symptoms.
The most common andropause symptoms include:
- depression
- loss of sex drive
- erectile dysfunction
- mood swings and irritability
- anger
- loss of muscle mass and reduced ability to exercise
- fat redistribution, such as developing a large belly or “man boobs” (gynaecomastia)
- a general lack of enthusiasm or energy
- difficulty sleeping an/or or increased tiredness
- night sweats
- hot flashes
- poor concentration and short-term memory challenges.
The most common male menopause symptoms include:
- depression,
- loss of sex drive,
- erectile dysfunction
- mood swings and irritability
- anger
- loss of muscle mass and reduced ability to exercise
- fat redistribution, such as developing a large belly or “man boobs” (gynaecomastia)
- a general lack of enthusiasm or energy
- difficulty sleeping an/or or increased tiredness
- night sweats
- hot flashes
- poor concentration and short-term memory challenges.
Many men will experience male menopause symptoms in their midlife, starting in their late 40s and 50s.
For true diagnosed andropause, caused by low testosterone levels, the treatment is testosterone replacement therapy (TRT). Many men experiencing andropause symptoms, however, are not actually low in testosterone. In these cases, lifestyle changes such as improving diet, sleep, and exercise habits as well as treatment for any anxiety, stress or depression will help manage or even correct the symptoms.
Yes, they can be. They may be caused by low testosterone, but more commonly they result from anxiety and/or stress, medication side-effects, alcohol consumption, diet, or a side effect of sleep apnea.
Yes, they can be. They may be caused by low testosterone, but more commonly they result from anxiety and/or stress, medication side-effects, alcohol consumption, diets, or a side effect of sleep apnea.
Compiled References
[1] https://www.nhs.uk/conditions/male-menopause/
[2] Singh P. Andropause: Current concepts. Indian J Endocrinol Metab. 2013 Dec;17(Suppl 3):S621-9. doi: 10.4103/2230-8210.123552. PMID: 24910824; PMCID: PMC4046605.
[3] https://www.merithealthcentral.com/health-library/128
[4] https://www.webmd.com/men/guide/male-menopause
[5] https://www.healthline.com/health/what-causes-night-sweats-in-men#common-causes
[6] https://www.healthline.com/health/mens-health/hot-flashes-men#symptoms
[7] https://www.forbes.com/health/mind/midlife-crisis/
[7a] https://www.webmd.com/men/features/mens-midlife-crisis
[7b] https://psychcentral.com/lib/midlife-crises-affecting-men-and-families
[7c] Infurna FJ, Gerstorf D, Lachman ME. Midlife in the 2020s: Opportunities and challenges. Am Psychol. 2020 May-Jun;75(4):470-485. doi: 10.1037/amp0000591. PMID: 32378943; PMCID: PMC7347230.
[8] https://www.healthline.com/health/cbt-techniques
[9] https://www.nimh.nih.gov/health/topics/anxiety-disorders#part_2225
[10] https://www.psychologytoday.com/ca/basics/anger
[11] https://www.medicalnewstoday.com/articles/cognitive-restructuring
[12] https://mantracare.org/therapy/anger/anger-management-counseling
[13] https://www.mayoclinic.org/diseases-conditions/erectile-dysfunction
[14] https://my.clevelandclinic.org/health/drugs/10053-vacuum-constriction-devices
[15] https://www.urologyhealth.org/urology-a-z/e/erectile-dysfunction-(ed)
[17] https://www.mayoclinic.org/healthy-lifestyle/sexual-health/expert-answers/loss-of-sex-drive
[18] Nandy PR, Singh DV, Madhusoodanan P, Sandhu AS. Male Andropause : A Myth or Reality. Med J Armed Forces India. 2008 Jul;64(3):244-9. doi: 10.1016/S0377-1237(08)80105-0. Epub 2011 Jul 21. PMID: 27408157; PMCID: PMC4921612.
[19] Bhasin S, Valderrábano RJ, Gagliano-Jucá T. Age-Related Changes in the Male Reproductive System. [Updated 2022 Feb 10]. In: Feingold KR, Anawalt B, Boyce A, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK278998/
[20] https://www.mayoclinic.org/healthy-lifestyle/mens-health/in-depth/male-menopause/art-20048056
Not AI generated.
Original content, last updated March 14, 2023.
© 2024 Herstasis® Health Foundation