What is Urinary Incontinence?
Urinary incontinence (UI), or bladder leakage, is the involuntary loss of urine. Urinary incontinence can occur during perimenopause and postmenopause when the muscles that keep the urethra closed weaken due to decreasing estrogen. Note that this can happen at other life stages due to lack of exercise resulting in muscle atrophy. In fact, one quarter to one third of men and women in the US experience symptoms of UI, most of them not in the menopausal transition. Urinary incontinence may also be associated with recurrent urinary tract infections (UTIs). [1] [2] [3] [4]
There are several types of urinary incontinence:
Stress incontinence:
Involuntary loss of urine when coughing, sneezing, laughing, jumping or lifting heavy objects. Stress UI can also occur when the pelvic floor is weakened, damaged or as a complication of obesity. [1] [5]
Urge incontinence:
When muscles in the bladder’s wall don’t work properly, there is an urgent need to urinate that cannot be controlled in time to make it to the toilet. Urge UI has multiple potential causes, ranging from diminished estrogen during perimenopause, an infection, diabetes, or as a complication of obesity. [1] [2]
Overflow incontinence:
when your bladder doesn’t fully empty when you urinate, you may experience frequent or even constant dribbles of urine. Be sure to give yourself enough time on the toilet to fully clear your bladder each time. [1] [6]
Women may be reluctant to speak up and act on UI issues due to embarrassment and/or negative feelings about aging. However, these conditions can usually be treated at home, or with the help of a trusted medical practitioner.

Self-care & Natural Remedies for Urinary Menopause Incontinence
You can take significant steps to treat incontinence on your own with some straightforward lifestyle changes. [1] [7]
- Strengthen your pelvic floor muscles through Kegel exercises. Make sure your Kegel exercises are done correctly as they can otherwise cause some harm. Talk to your medical care provider or find a physiotherapy that specializes in pelvic floor exercises. [8]
- Try bladder training through a combination of scheduled bathroom visits and delayed urination
- Keep a journal to identify and monitor triggers
- Reduce intake of caffeine and diuretics to minimize excess urine production
- Find the right balance of fluid intake. Drinking too much or too little can make incontinence much worse.
- Empty your bladder before bedtime to promote an uninterrupted night of sleep
- For added peace of mind when out in public, use pantiliners or pads for extra protection. There are also now many brands of comfortable but absorbent protective underwear.

Therapy & Treatment for Urinary Menopause Incontinence
Therapy for UI will vary depending on the type and the severity of the incontinence you are experiencing. It will also depend on risk factors you have, such as obesity, in addition to experiencing the menopausal transition. [1]
It is important to find a reliable, educated primary care provider familiar with recognizing and treating the symptoms of perimenopause and menopause. The North American Menopause Society provides a list of menopause practitioners here. Developing a trusting relationship with a healthcare provider will also help reduce the potential embarrassment you may feel admitting to UI. [12]

Behavioural changes to help UI:
- Bladder training works by consciously delaying urination once you have the urge to pee. The length of the delay will increase progressively, giving you more confidence about holding your bladder till you can reach the toilet. Scheduling trips to the bathroom can also be helpful – set a timer and urinate every few hours rather than waiting for the urge.
- Practice ‘double voiding’ to make sure your bladder is completely empty: wait a few moments once you’ve finished peeing and then try again, to make sure all the urine is out.
Exercise to help UI:
- Kegels, or pelvic floor exercises, can help control incontinence, especially stress incontinence. You may ask for a referral to a physiotherapist who specializes in pelvic floor training.
Medications to help UI:
- Menopausal transition UI can be treated with topical estrogen, but will need to be tailored to the type of incontinence you are experiencing.
Medical devices to help UI:
- A urethral insert can be placed into the urethra before an activity (such as exercise) to essentially serve as a plug, like a tampon, and prevent leakage.
- A flexible silicone ring called a Pessary can be inserted into the vagina for the day to help support the urethra and prevent leakage.
Sources: [1] [2] [3] [8] [9]
If none of these therapies work for you, there are several surgical techniques that will resolve incontinence. Speak to your healthcare provider to see if any would be applicable to you.
The Science
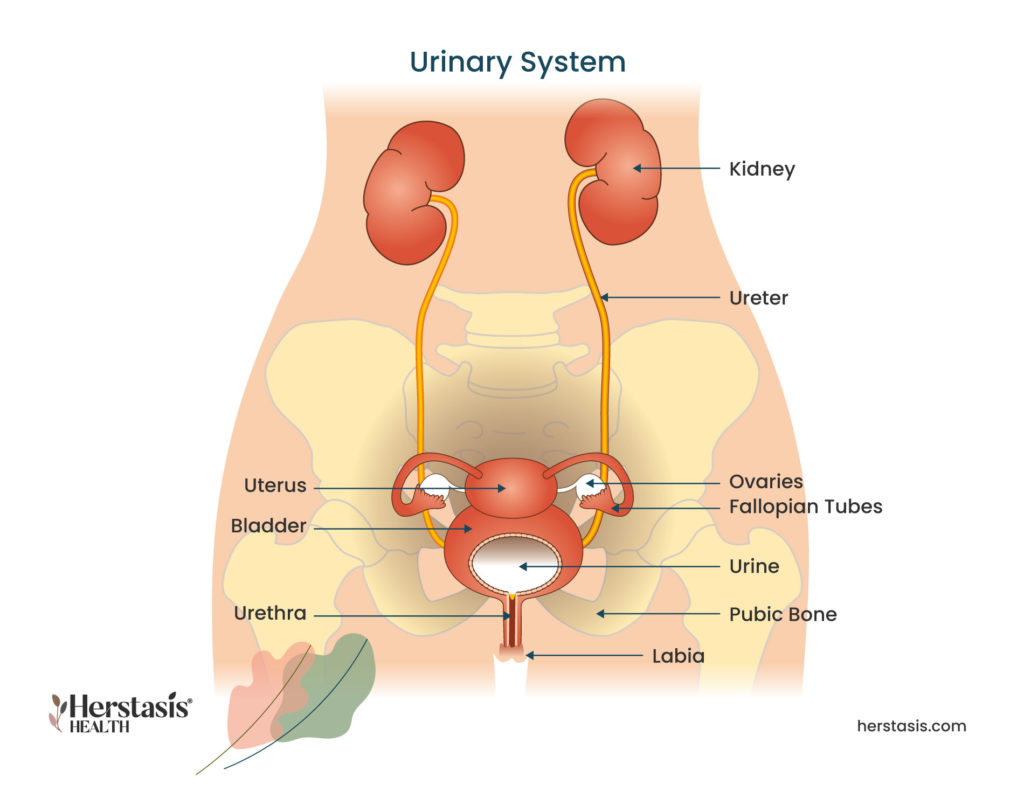
Urinary leakage, or incontinence, can have multiple causes, some of which can occur as a result of changes in hormone levels. Like many female tissues, the hormone estrogen impacts the lining of the urethra, which is the tube that carries urine from the bladder so it can be excreted out of the body. During the menopausal transition, this lining thins and weakens so that it gives in to the pressure from the urine in the bladder. This leads to involuntary leakage of urine.
Other common causes of female incontinence include weakening of the muscles that support the bladder, injuries that happened during childbirth or another traumatic event, and changes to the uterus that could cause it to press down on the bladder.
Download
Genitourinary Syndrome of Menopause (GSM)
Changes to the vagina usually occur at the same time as changes in the urinary tract, so they have recently been combined into a single category – genitourinary syndrome of menopause (GSM). GSM covers a variety of changes to the genitourinary tract – particularly the urethra, vagina and vulva. Vaginal atrophy and urinary incontinence (UI) are the most common symptoms of GSM, affecting 40-50% of midlife and aging women. [10] [11]
Signs and Symptoms of GSM
| Vagina | |
| – | vaginal dryness |
| – | irritation / burning / itching |
| – | changes to vaginal discharge |
| – | thinning / graying pubic hair |
| – | vaginal / pelvic pain and pressure |
| – | vaginal prolapse (top of the vagina falling into the vaginal canal) |
| Urinary System | |
| – | painful urination |
| – | urgency incontinence |
| – | stress incontinence |
| – | frequent / recurring urinary tract infections |
| – | urethral prolapse |
| Sexual | |
| – | painful sex |
| – | bleeding after sex |
| – | decreased orgasm |
| – | loss or reduction in libido |
| – | pain after orgasm (dysorgasmia) |
Statistics


Yes, the vaginal atrophy part of GSM can be helped by regular sexual activity with or without a partner! Increasing blood flow to the vagina will help keep the tissues healthy. Bladder training and strengthening the pelvic floor muscles with Kegels are helpful to naturally manage urinary incontinence. While these may not be enough to completely manage GSM, they are a good start.
Unfortunately, no. The Genitourinary Syndrome of Menopause is a chronic progressive condition related to aging and reduced levels of estrogen. Menopause Hormone Therapy (MHT) can be highly effective to slow the progression of GSM. Check with your healthcare provider.
The lining of the outer urethra is estrogen-dependent. During the menopausal transition, this lining thins and may become weaker than the pressure in the bladder. It is this imbalance that leads to involuntary loss of urine.
Read more on the science here
The lining of the outer urethra is estrogen-dependent. During the menopausal transition, this lining thins and may become weaker than the pressure in the bladder. It is this imbalance that leads to involuntary loss of urine.
Check out the science here
Urine leakage can also be caused by damage done to the urethral sphincter during childbirth, as a complication of obesity and as a side-effect of urological surgeries such as a hysterectomy.
YES
Kegel exercises, done routinely, help with stress incontinence in most women. It is helpful to do Kegel contractions when exercising, walking, stretching or during yoga.
Compiled References
[1] https://www.urologyhealth.org/urology-a-z/u/urinary-incontinence
[2] https://my.clevelandclinic.org/health/diseases/22161-urge-incontinence
[3] Kołodyńska, G., Zalewski, M., & Rożek-Piechura, K. (2019). Urinary incontinence in postmenopausal women – causes, symptoms, treatment. Przeglad menopauzalny = Menopause review, 18(1), 46–50. https://doi.org/10.5114/pm.2019.84157
[4] Bulan, S. E. (2019). Physiology and Pathology of the Female Reproductive Axis. In Melmed, S., Koenig, R., Rosen, C., Auchus, R. & F. Goldfine (Eds.), Williams Textbook of Endocrinology (14th ed., pp. 574-641). Elsevier.
[5] https://www.mayoclinic.org/diseases-conditions/stress-incontinence/symptoms-causes
[6] https://www.webmd.com/urinary-incontinence-oab/overflow-incontinence
[7] https://www.mayoclinic.org/diseases-conditions/stress-incontinence/diagnosis-treatment/drc-20355732
[8] Dumoulin, C., Cacciari, L. P., & Hay-Smith, E. (2018). Pelvic floor muscle training versus no treatment, or inactive control treatments, for urinary incontinence in women. The Cochrane Database of Systematic Reviews, 10(10), CD005654. https://doi.org/10.1002/14651858.CD005654.pub4
[9] Krause, M., Wheeler, T. L., 2nd, Richter, H. E., & Snyder, T. E. (2010). Systemic effects of vaginally administered estrogen therapy: a review. Female pelvic medicine & reconstructive surgery, 16(3), 188–195. https://doi.org/10.1097/SPV.0b013e3181d7e86e
[10] https://www.mayoclinic.org/diseases-conditions/vaginal-atrophy
[11] Angelou K, Grigoriadis T, Diakosavvas M, Zacharakis D, Athanasiou S. The Genitourinary Syndrome of Menopause: An Overview of the Recent Data. Cureus. 2020 Apr 8;12(4):e7586. doi: 10.7759/cureus.7586. PMID: 32399320; PMCID: PMC7212735.
[12] Sheryl A. Kingsberg, Jonathan Schaffir, Brooke M. Faught, JoAnn V. Pinkerton, Sharon J. Parish, Cheryl B. Iglesia, Jennifer Gudeman, Julie Krop, and James A. Simon. Female Sexual Health: Barriers to Optimal Outcomes and a Roadmap for Improved Patient–Clinician Communications. Journal of Women’s Health. 2019 28:4, 432-443 doi: 10.1089/jwh.2018.7352