What is Body Pain?
There are many different causes of pain in your body, many different experiences of pain (such as throbbing, stabbing, aching, or pinching) and many different approaches to treating pain.
Medically, pain is classified based on the nerve pathways that are used to signal the brain. The first type is called nociceptive pain, which results from the stimulation of specialized nocioceptor cells. The second type is called neuropathic pain, which results from the stimulation of any nerve cells, not just the nocioceptor cells. This is important to understand as these types of pain have different causes and therefore different treatment approaches.
Nocioceptive Pain
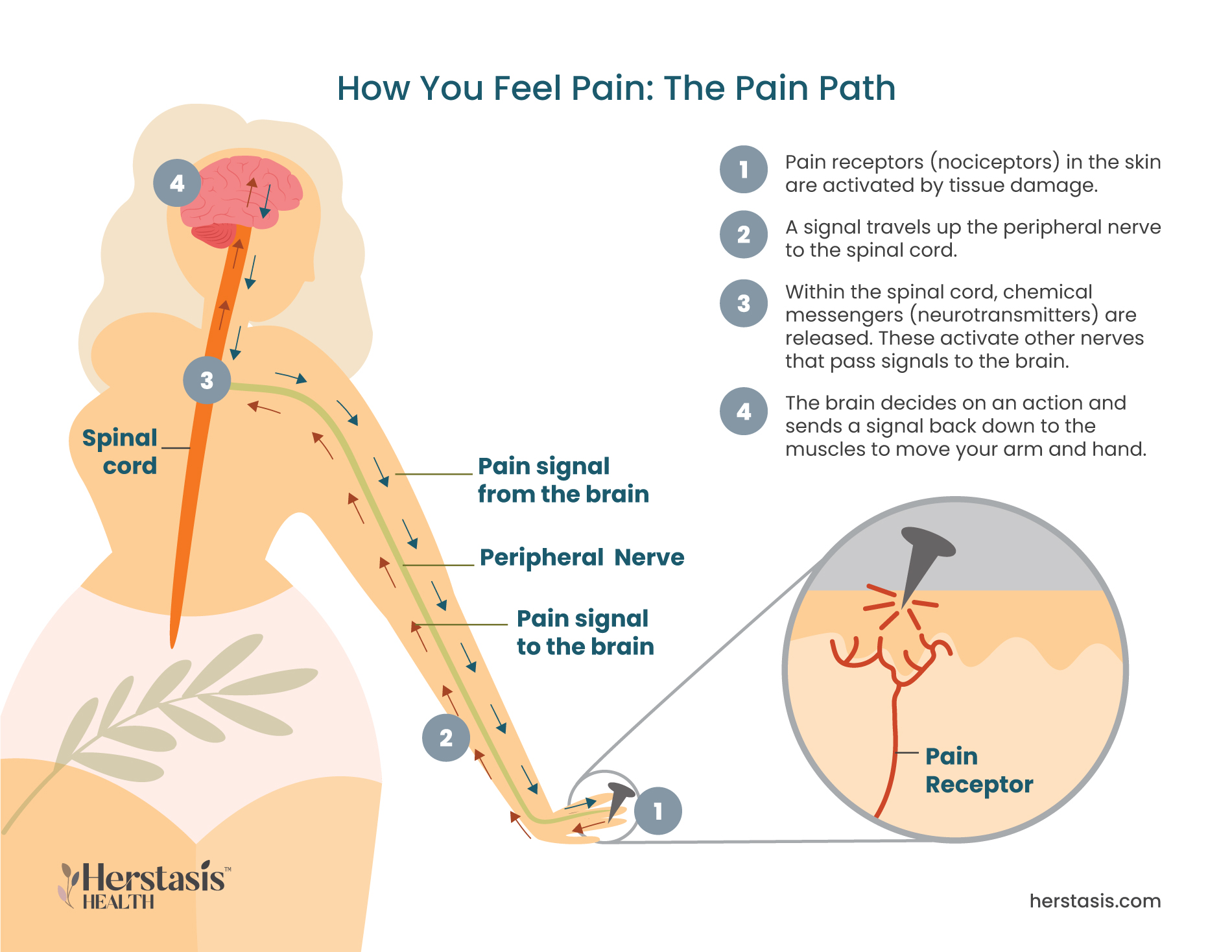
Nociceptors are specialized nerve cells located on the surface of the skin and throughout most of the body. These receptors are highly sensitive and detect changes in temperature or pressure, and the presence of toxic or injury-causing chemicals.
Nociceptive pain is caused by any damage to body tissues that activates the nociceptors through a direct stimulus. Once they are activated, the nociceptors transmit signals to the brain that cause a protective response. For example, if the nociceptors detect an extreme temperature and signal your brain, your brain will, in turn, signal your muscles to pull your hand away from the stove. Nociceptive pain goes away when the stimulus (in this example, the hot temperature) stops. [1]
Neuropathic Pain
Neuropathic pain is caused by damage or dysfunction (such as inflammation, irritation, or neural tissue compression) within the nervous system itself. The damaged nerve cells can send spontaneous signals to the brain that are interpreted and felt as pain or the damaged cells can amplify normal pain responses.
Neuropathic pain can be experienced long-term or it can be resolved more quickly if the underlying damage is repaired. For example, if a tumour is pressing on nerve cells that will cause them to send pain signals to the brain. If treatment of some sort shrinks the tumour so it stops pressing on the nerve cells, the pain will stop. Unfortunately, many causes of chronic neuropathy are not easy to diagnose and so they are not easy to fix.
Nociceptor pain can become neuropathic pain. The nocioceptors stop signalling pain once the stimulus is removed, but the stimulus event may have caused underlying damage to the tissues. This damage can then affect the nerves in the same way as neuropathic pain. For example, if you twist your ankle, the nocioceptors will fire and you will feel pain because your ankle ligaments moved in a way they are not designed to move. However, damage to the ligaments will have caused swelling and inflammation, and that will trigger your nerves to send pain signals. You will continue to feel pain until the underlying damage is healed.
Regardless of internal nervous system pathways, pain is also classified as either acute or chronic pain. Acute pain happens quickly based on a clear stimulus and it goes away when the stimulus stops. Stubbing your toe is a type of acute pain. Your toe hits a hard object and the pain starts immediately. Chronic pain, on the other hand, doesn’t always have a clear cause and there is no obvious external stimulus. Pain is diagnosed as chronic when it lasts for more than six months.
Emerging evidence is showing that hormone changes during the menopausal transition create inflammation throughout the body. In addition to its role in the reproductive system, estrogen is a ‘master regulator’ impacting multiple female body systems. For example, estrogen protects the body from insulin resistance and type II diabetes as well as regulating metabolism. Estrogen also regulates inflammasomes, which are a key part of the immune response and that are responsible for the activation of inflammatory responses. [9]
During the menopausal transition, some women find that they experience pain – either new pain or more pain than usual – in different areas of their bodies. This pain is almost always neuropathic pain and it happens because lowered levels of estrogen are associated with chronic low-grade inflammation. Inflammation results in the buildup of fluid that pushes against nerve endings and results in neuropathic pain of various types (constant, throbbing, etc.) and severity. It appears that changes in estrogen levels, not the absolute levels themselves, are associated with increased levels of pain. [8]

Joint and Muscle Pain and Stiffness
Many women experience joint and muscle pain and stiffness around the time of menopause, and in many cases this is pain that they haven’t experienced before. There are many causes of joint pain, and for mid-life women, hormones play a significant role. Estrogen helps to lower inflammation, so decreasing levels of estrogen during the menopausal transition are associated with increased levels of inflammation throughout your body. This inflammation can add to the existing pain caused by old joint and muscle injuries, wear and tear, and just plain aging or it can trigger pain in joints that haven’t hurt before. This is a type of neuropathic pain and can become chronic. [2]

Breast Pain
Breast pain is common for many women as part of their menstrual cycles and it results from hormone activity. Estrogen and progesterone both increase during the second half (days 14 to 28) of a typical 28 day menstrual cycle. Estrogen causes the breast ducts to get larger and progesterone causes the milk glands to swell. This type of neuropathic pain can cause your breasts to feel painful, tender, and swollen.
The changing hormone levels during the menopausal transition alter your regular cycle and this in turn alters the effects of estrogen and progesterone on your breasts. While menopause sore breasts may not be much different from your normal monthly episodes of breast tenderness, irregular menstrual cycles means that breast tissue is also affected at unpredictable times and for unpredictable durations. [3]

Fibromyalgia
Women diagnosed with fibromyalgia experience widespread body pain as well as sleep problems, fatigue, depression, and headaches. The cause of fibromyalgia is not known. For women diagnosed with fibromyalgia, the menopausal transition can increase typical levels of pain because of the fluctuation in estrogen levels and the impact those fluctuations can have on inflammation.
Fibromyalgia is a chronic pain condition that is often diagnosed for the first time in women entering the menopausal transition. Some symptoms of the menopausal transition, like increased pain, fatigue, and/or vaginal dryness, can overlap with those associated with fibromyalgia. This can make a new diagnosis of fibromyalgia difficult because the root cause of the symptoms may not be clear. [2a]

Dyspareunia or Pain During Sex
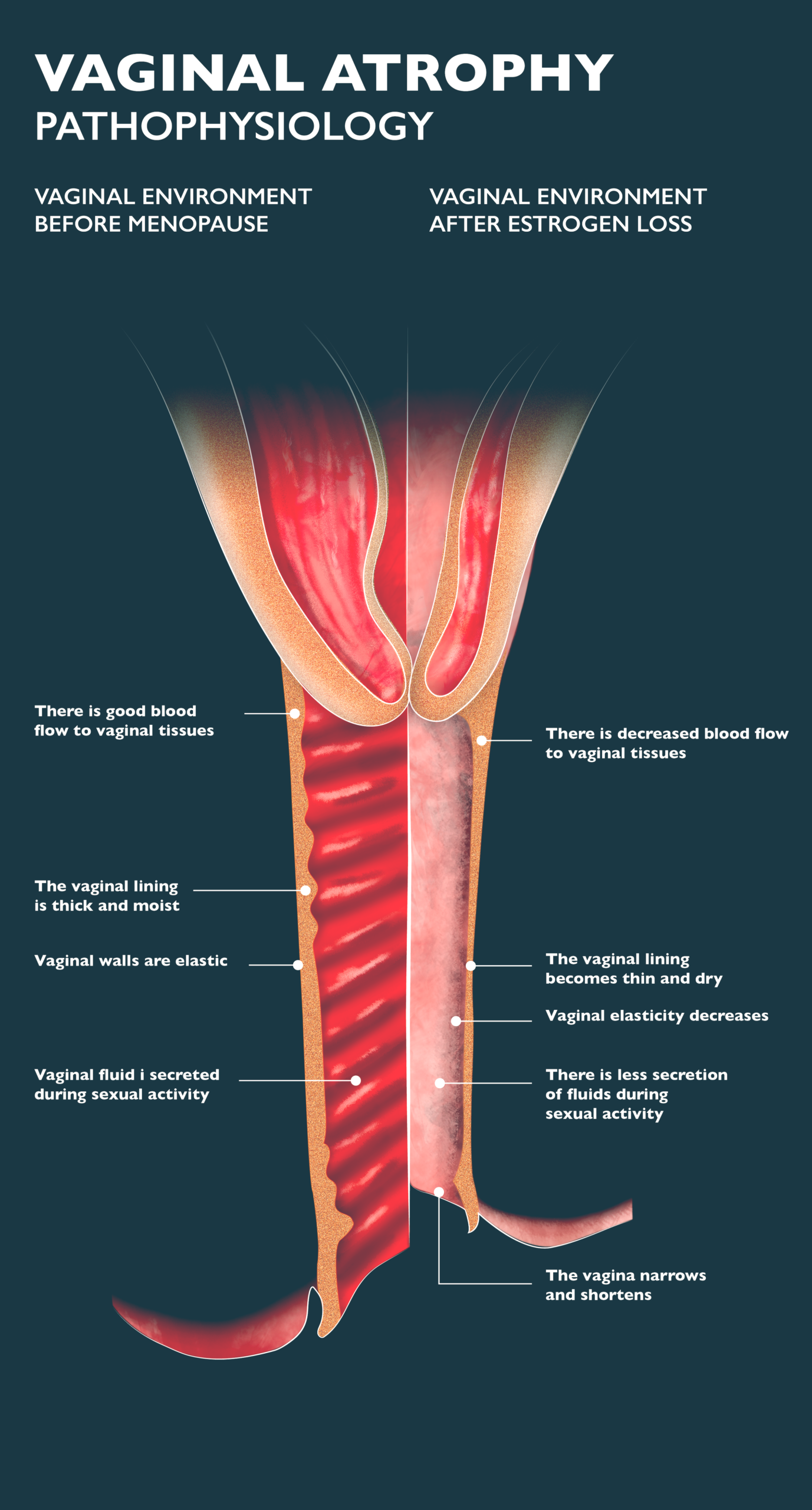
The lower levels of estrogen seen during the menopausal transition may cause changes to your vaginal tissues – they get thinner, dryer, and may get inflamed, causing pain, burning, or discharge. When this happens, the nociceptors will respond with pain signals, particularly during penetration and intercourse. symptoms of a condition called vaginal atrophy. Sadly dyspareunia is not rare and between 17% and 45% of postmenopausal women say they find sex painful.
Another cause of pain during sex is vulvodynia, where women experience chronic pain in the vulva (the external part of female genitals). There is no clear cause for the pain, making it neuropathic. This condition can last for years and there is no consistent treatment for it. You can work with your healthcare provider to develop a customized treatment and management plan.
Self-care & Natural Remedies for Body Pain
You can work to reduce any body pain you may be experiencing with these simple, easy steps:
- Get Regular Exercise. It may seem counter-intuitive, but regular exercise is very important in the management of joint and muscle pain. Exercising consistently and choosing low-impact exercise such as swimming, biking, hiking, and yoga, can help reduce the pain and stiffness in your joints and help prevent further problems.
- Take a forest bath. Or at least get out into natural outdoor environments. This, coupled with gentle exercise and mindfulness, can be an effective way to manage pain using the power of nature.

- Eat a Healthy Diet. Eating a healthy, balanced diet gives you the nutrients you need to cope with pain during the menopausal transition. Your diet can also be customized to manage specific types of pain. For example, omega-3 fatty acids are known to have anti-inflammatory effects. Increasing your intake of salmon, mackerel, sardines, or trout, or nuts and seeds containing omega-3 fatty acids can help ease inflammation in your joints and decrease the pain. These can also be taken in the form of supplements for menopause joint pain.
- Consider getting massage therapy, acupuncture, heat or cold application, or hypnosis. All of these can be effective for pain reduction, but you may need to try different types of treatment to find the ones that work best for you.
- Consider seeing a therapist or a counselor. Many types of therapy, including cognitive behavioural therapy (CBT), group therapy, and psychological counseling can help manage your pain.
- Meditation, relaxation, breathing and mindfulness exercises can be effective in managing pain. Talk to your healthcare provider or seek out a yoga or meditation studio that can provide guidance and community resources.
- If you smoke, or have other unhealthy habits, work to quit. Quitting bad and unhealthy habits can increase positive feelings, improve circulation, and reduce stress, all of which may help to reduce pain.
- If your breasts hurt, get a properly-fitting bra. One study showed that 85% of women with breast pain gained relief when they wore a well-fitted sports bra. To fit your bra properly, go to a professional lingerie fitter, or follow these guidelines and make sure that:
- your bra feels comfortable;
- the back of the bra doesn’t slide up your back;
- the shoulder straps do not dig into your shoulders;
- your nipple is at the same level as a line midway between your shoulder and elbow;
- your breasts fit inside the cups and don’t bulge out above the cups or into your armpits;
- if you prefer underwire bras, the underwire lies flat against the body and doesn’t dig in anywhere;
- your finger can easily fit under the band, ensuring it isn’t too tight around your ribcage; and
- the centre of the bra in front sits close to your breast bone (sternum).
- Relaxation techniques or gently massaging over-the-counter pain cream into sore breasts has been shown to be helpful for up to 60% of women.
- For vaginal pain, use over-the-counter lubricants to hydrate the walls of your vagina. This can also help reduce vaginal infections.
- Keep your vaginal tissues healthy by stimulating the muscles of the vagina and increasing the blood flow to the vaginal wall with vaginal sex and masturbation.
- Avoid vaginal intercourse when experiencing pain and dryness, as this can result in tearing delicate tissues and may lead to infections.
Therapy & Treatment for Body Pain
At age 40 find a reliable, educated primary care provider familiar with recognizing and treating symptoms of perimenopause and menopause. The North American Menopause Society provides a list of menopause practitioners here.
If your pain is sudden, new, or extreme, make sure you tell your health-care provider as pain can have many causes beyond changing hormones. Track your pain, including where and when it happens and how intense the pain is, and communicate these to your healthcare provider.
There are multiple approaches to treating and managing chronic pain. The Practice Guidelines for Chronic Pain Management from the American Society of Anesthesiologists [13] recommend the following:
Multimodal interventions use more than one (= multi-) type (= modal) of therapy for the treatment of chronic pain. Multidisciplinary interventions are multimodal approaches that come from more than one field of study (e.g. psychological; surgical; pharmacological etc.) Research has shown that using multidisciplinary treatment programs can be effective in reducing the intensity of pain reported by patients for periods of time ranging from 4 months to 1 yr when compared to treatments from a single discipline.

Multimodal Intervention (combined therapies)
Multimodal Intervention
Multimodal interventions should be part of a treatment strategy for patients with chronic pain. The following are individual treatments from multiple disciplines that can be combined into personalized multimodal treatments, following the guidance of your healthcare provider:
- Ablation – Ablative techniques involve the removal or destruction of a body part or tissue or its function. Ablative procedures include denervation, which is the removal of nerves.
- Acupuncture -Studies with observational findings indicate that acupuncture can provide pain relief for assessment periods of 1 week to 6 months.
- Nerve and nerve root blocks – Blocks are injections of medication into a group of nerves that are causing chronic pain. Observational studies indicate that the improvement in pain scores over the baseline pain scores can last one to six months.
- Botulinum toxin (botox) – Botulinum toxin or botox comes from a bacterium called Clostridium botulinum. It works by blocking neuromuscular signals. Botox prevents the release of a type of neurotransmitter called acetylcholine from motor nerves, a process termed chemical denervation. When the nerves are not functioning, they do not trigger any pain signals.
- Neuromodulation with Electrical Stimulus – Neuromodulation is a technique that alters nerve activity by delivering electrical impulses directly to the target area. Observational studies indicate that neuromodulation of peripheral nerves under the skin (subcutaneous) can provide pain relief for periods ranging from 4 months to 2 years. Neuromodulation on the spinal cord can be effective for chronic radiating pain (radicular pain) that occurs from multiple causes (e.g. neuropathic pain, spinal cord injury, etc.)
- TENS (transcutaneous electrical nerve stimulation) – A TENS machine is a device that allows you to connect electrodes to your skin in areas that are painful. The machine delivers small electrical impulses to your skin, which you feel as a tingling sensation. Observational findings show that TENS results in improved pain scores for a variety of pain conditions for three to six months
- Physical and/or restorative therapy – Working with a physical therapist is recommended for all chronic pain conditions.
- Psychological treatments / therapies – These include cognitive behavioral therapy (CBT), biofeedback, and relaxation training as well as psychotherapy, group therapy, or counselling. Randomized controlled trials (RCTs) indicate that these therapies can provide relief of back pain or other chronic pain conditions for up to two years. [13]
Therapy & Treatment for Joint Pain or Muscle Stiffness
Therapy & Treatment for Joint Pain & Muscle Stiffness
Estrogen-only hormone therapy may be helpful in stabilizing your hormone levels and decreasing the inflammation throughout your body. One study that came out of the Women’s Health Initiative (WHI) trials analyzed 10,000+ post-menopausal women. The baseline condition of women in randomized groups showed 77% of these women reported joint pain. The study compared treatment with estrogen-only therapy vs no treatment (placebo). After one year, the frequency of joint pain was significantly lower among women who received estrogen-only therapy, compared to women who were in the placebo group (76.3% s. 79.2%). The study was extended and after three years, the women who received the estrogen-only therapy continued to have less frequent joint pain than the placebo group. The study concluded that estrogen-alone therapy in postmenopausal women resulted in modest but sustained improvements in the frequency of joint pain. Combined estrogen and progesterone therapy was not part of the clinical trial, so the results reported here apply to estrogen-only hormone therapy. [4]
Therapy & Treatment for Painful Sex
Therapy & Treatment for Painful Sex
Topically (locally) applied hormone therapy (HT) with estrogen is safe and often effective for reducing dryness in the vaginal lining and improving strength of the vaginal wall. Topical HT comes in the form of creams to apply inside the vagina or tablets and rings that can be placed inside the vagina. Locally applied estrogen can also help to reduce the incidence of urinary tract infection.

Therapy & Treatment for Vaginal Pain
Therapy & Treatment for Vaginal Pain
Vulvodynia is chronic pain or discomfort around the opening of your vagina (vulva) that has no identifiable cause and that lasts for at least three months. [4a] The treatment for vulvodynia is variable and the best course of therapy requires trying different treatments until one or a combination of several treatments (multi-modal) provides relief. The treatment options include:
- Medications, including steroids or anticonvulsants may help lessen chronic pain. Antihistamines can be used to reduce itching if that is one of your symptoms.
- Biofeedback therapy, which can provide you with the skills to relax your pelvic muscles and better control your responses to the pain.
- Local or topical anesthetics, which are particularly useful to reduce pain in advance of intercourse. If you do use an anesthetic, note that it can affect your partner who may experience temporary numbness after intercourse.
- Nerve blocks, which are used if you don’t respond to other treatments.
- Pelvic floor therapy, as vulvodynia is associated with tension in the muscles of the pelvic floor. If this tension can be relieved it may help manage or eliminate the pain.
- Surgery is a last resort. This type of ablation removes the affected skin and tissue around the vulva and can provide long-term relief for some women.
The Science

Estrogen, Testosterone and Pain
Estrogen, Testosterone and Pain
There are well recognized sex differences in how pain is experienced. A number of studies have shown that women experience more chronic pain issues and have greater pain sensitivity compared to men. It is important to recognize that while pain sensitivity is affected by biological factors, it is also affected by social, cultural and psychological factors. The biological factors are sex hormones like estrogen and testosterone. These influence pain sensitivity, with multiple study results showing that women’s pain thresholds and pain tolerances vary depending on the stage of their menstrual cycle.[5][6]
Motor Nerve Conduction Velocity (MNCV) is used as a reliable and quantitative method to assess the status of fast-conducting peripheral motor nerve fibres, the types of nerve cells involved in neuropathic pain. One study explored the relationship between peripheral motor nerve status and hormone levels by comparing MNCV in post-menopausal women with peripheral neuropathy to post-menopausal women without peripheral neuropathy (the control subjects) and then correlating MNCV with estrogen and progesterone levels. The results showed that post-menopausal women with peripheral neuropathy had significantly lower estrogen and progesterone levels compared to control subjects. [7]
The role of estrogen in pain is complicated. During the menstrual cycle, pain is most common when estrogen is at its lowest levels. However, girls report more pain than boys from the onset of puberty when estrogen starts to rise. Researchers have concluded that changes in hormone levels are the problem, rather than the absolute levels themselves. [8]

Peripheral Nervous System vs Central Nervous System
Peripheral Nervous System vs Central Nervous System
Pain is experienced due to the action of your nervous system. When nerve cells are stimulated by a stimulus, they send a signal along the nervous system pathway that is received by your brain. Your brain in turn sends a response signal back down the nervous system pathway.
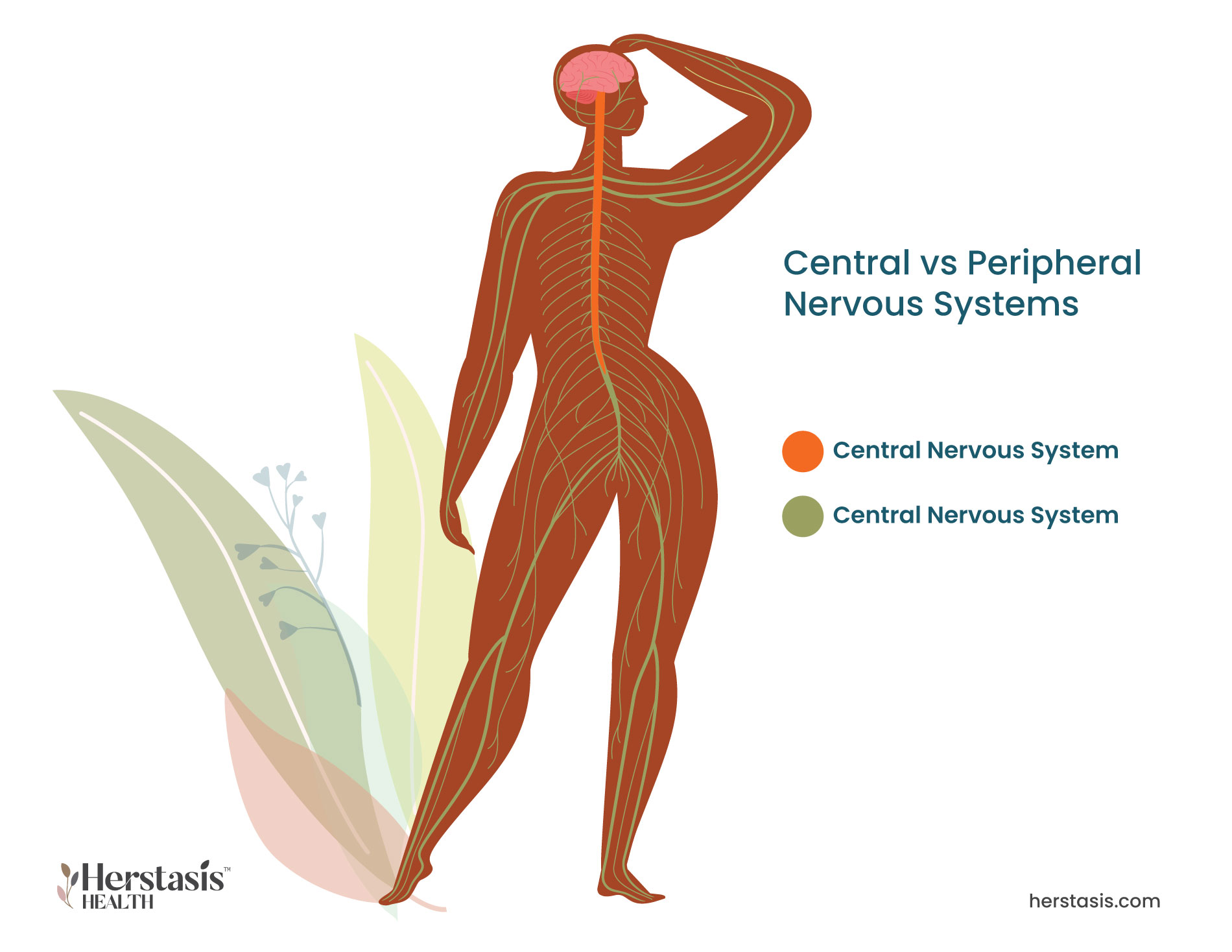
Your central nervous system is made up of your brain and your spinal cord. Your peripheral nervous system is made up of all of the nerves that are located outside of the central nervous system. The two types of pain, nociceptive and neuropathic, can be differentiated by the origin of the pain signal. Nociceptive pain always originates in the peripheral nervous system because there are no nociceptors in the central nervous system. Neuropathic pain may originate in the peripheral or the central nervous system. Neuropathic pain is caused by inflammation, irritation or neural tissue compression, whereas nociceptive pain is a response to a specific trigger or stimulus.
During the menopausal transition, some women find that they experience pain – either new pain or more pain than usual – in different areas of their bodies. This pain is almost always neuropathic pain and it happens because lowered levels of estrogen are associated with chronic low-grade inflammation. Inflammation results in the buildup of fluid that pushes against nerve endings and results in neuropathic pain of various types (constant, throbbing, etc.) and severity. It appears that changes in estrogen levels, not the absolute levels themselves, are associated with increased levels of pain. [8]
[8] Dennis, C. Surging hormones blamed for pain. Nature (2005). https://doi.org/10.1038/news050822-6
Breast pain is common for many women as part of their menstrual cycles and it results from hormone activity. Estrogen and progesterone both increase during the second half (days 14 to 28) of a typical 28 day menstrual cycle. Estrogen causes the breast ducts to get larger and progesterone causes the milk glands to swell. This type of neuropathic pain can cause your breasts to feel painful, tender, and swollen.
The changing hormone levels during the menopausal transition alter your regular cycle and this in turn alters the effects of estrogen and progesterone on your breasts. While the pain itself may not be much different from your normal monthly episodes of breast tenderness, irregular menstrual cycles means that breast tissue is also affected at unpredictable times and for unpredictable durations. [3]
[3] https://www.webmd.com/menopause/guide/breasts-menopause
Many women experience joint and muscle pain and stiffness around the time of menopause, and in many cases this is pain that they haven’t experienced before. There are many causes of joint pain, and for mid-life women, hormones play a significant role. Estrogen helps to lower inflammation, so decreasing levels of estrogen during the menopausal transition are associated with increased levels of inflammation throughout your body. This inflammation can add to the existing pain caused by old joint and muscle injuries, wear and tear, and just plain aging or it can trigger pain in joints that haven’t hurt before. This is a type of neuropathic pain and can become chronic. [2]
[2] https://www.healthline.com/health/menopause/pain#changes
MYTH
We are absolutely done with this thinking at Herstasis. Pain is a sign that there is a problem and the first step is to talk to your health-care provider. If they don’t treat your pain with compassion and empathy, find another health-care provider. Together you can come up with a plan to identify the source of your pain and then you can determine the best course of action.
MYTH
No. No. No. No. Pain is a sign that something is wrong, listen to your body. Pain can be treated, but there is no way to start treatment if you do not acknowledge the pain in the first place and seek help. Talk to your health care provider about your pain, track it over time to see if it is coupled with any other symptoms, and start a treatment plan. There are many healthy ways to manage chronic pain including professional counseling, support group meetings, mindfulness training and breathing exercises, meditation, and the use of various medical therapies, devices and techniques.
MYTH
Not True! Changes in estrogen levels can impact the levels of inflammation throughout the body, which can then increase pain in multiple parts of the body. But pain is not normal, it is a signal that something is wrong. Talk to your healthcare provider about any changes to the levels of pain you are experiencing. If the underlying cause can be identified then treating the source of the pain is possible. Even if there is no clear cause, such as with fibromyalgia, your healthcare provider can help you find ways to manage the pain. Practicing self-care as outlined in the above material can also make a big difference.
MYSTERY
Research supports the fact there is a gender difference in the way pain systems function. Studies have found that there is a higher density of nerves in women that may cause a greater sensitivity to pain. The pain itself may be at a similar level but the perception of pain is different, with women perceiving more pain than men for similar stimuli. [12]
A fascinating study on pain and sex hormones looked at a unique study group – individuals undergoing sex-change procedures. One research trial showed that 30% of men who started taking female hormones began experiencing chronic pain during their treatment. When women started taking testosterone as part of their sex-change transition, more than half reported a reduction in their chronic pain. [8] The underlying processes around how sex hormones impact pain tolerance are poorly understood at the moment. Researchers propose that testosterone somehow reduces or blocks the pain signaling pathways in the central nervous system. Conversely, estrogen reverses this and stops any blockage of pain signals so pain sensitivity appears to increase. [8]
FALSE
This is not true. Sensing pain is subjective so it is highly variable amongst individuals. There is also a clear difference between how men and and women experience pain. Recent research has shown that male and female [mice!] differ in the neural pathways to sensing pain. Male mice that lack testosterone experience the ‘female’ path, and females that lack T cells (special cells involved in the usual female pain transmission path) or are pregnant switch to the pathway seen in male mice. More research is underway to understand this better. [11]
Yes, this is a normal symptom.
As estrogen declines during the perimenopausal transition, inflammation in your system develops because estrogen modulates your immune system and the biochemical signals that cause inflammation. You may notice you are developing osteoarthritis in some of your joints, and old joint injuries may begin to hurt and become stiff. As well, some women may experience an increase in their auto-immune disease symptoms.
To date, it isn’t known whether standard HT with estrogen is helpful for joint pain and inflammation. However it is known that joint inflammation can be reduced by regular moderate exercise including modified strength training. Low- impact exercises such as swimming and cycling are excellent at reducing pain and inflammation, promoting high quality sleep and they won’t damage your spine, knees and hips.
Compiled References
[1] Dubin, A. E., & Patapoutian, A. (2010). Nociceptors: the sensors of the pain pathway. The Journal of clinical investigation, 120(11), 3760–3772. https://doi.org/10.1172/JCI42843
[2] https://www.healthline.com/health/menopause/pain#changes
[2a] https://www.cdc.gov/arthritis/basics/fibromyalgia
[3] https://www.webmd.com/menopause/guide/breasts-menopause
[4] Chlebowski RT, Cirillo DJ, Eaton CB, Stefanick ML, Pettinger M, Carbone LD, Johnson KC, Simon MS, Woods NF, Wactawski-Wende J. Estrogen alone and joint symptoms in the Women’s Health Initiative randomized trial. Menopause. 2013 Jun;20(6):600-8. doi: 10.1097/GME.0b013e31828392c4. PMID: 23511705; PMCID: PMC3855295.
[4a] https://www.mayoclinic.org/diseases-conditions/vulvodynia/symptoms-causes/syc-20353423
[5] Chen, Q., Zhang, W., Sadana, N. et al. Estrogen receptors in pain modulation: cellular signaling. Biol Sex Differ 12, 22 (2021). https://doi.org/10.1186/s13293-021-00364-5
[6] Wiesenfeld-Hallin Z. Sex differences in pain perception. Gend Med. 2005 Sep;2(3):137-45. doi: 10.1016/s1550-8579(05)80042-7. PMID: 16290886.
[7] Singh, A., Asif, N., Singh, P. N., & Hossain, M. M. (2016). Motor Nerve Conduction Velocity In Postmenopausal Women with Peripheral Neuropathy. Journal of clinical and diagnostic research : JCDR, 10(12), CC13–CC16. https://doi.org/10.7860/JCDR/2016/23433.9004
[8] Dennis, C. Surging hormones blamed for pain. Nature (2005). https://doi.org/10.1038/news050822-6
[9] McCarthy, M., Raval, A.P. The peri-menopause in a woman’s life: a systemic inflammatory phase that enables later neurodegenerative disease. J Neuroinflammation 17, 317 (2020). https://doi.org/10.1186/s12974-020-01998-9
[10] https://www.menopause.org/for-women/sexual-health-menopause-online/sexual-problems-at-midlife.
[11] Why the sexes don’t feel pain the same way. Nature 567, 448-450 (2019). doi: https://doi.org/10.1038/d41586-019-00895-3
[12] American Society of Plastic Surgeons. “Study Reveals Reason Women Are More Sensitive To Pain Than Men.” ScienceDaily. ScienceDaily, 25 October 2005. www.sciencedaily.com/releases/2005/10/051025073319.htm
[13] Practice Guidelines for Chronic Pain Management: An Updated Report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine. Anesthesiology 2010; 112:1–1
[14] https://www.practicalpainmanagement.com/how-can-botulinum-toxin-be-used-chronic-pain-syndromes