Perimenopause Anxiety Symptoms
What are Perimenopause Anxiety Symptoms?
Anxiety disorders are different from having occasional worries or fears. When you are experiencing an anxiety disorder, the anxiety does not go away and sometimes it continues to grow and keeps getting worse over time. Abnormal anxiety will interfere with daily activities, making work, relationships, and normal functioning difficult. [3]
Symptoms associated with anxiety are commonly felt in the chest or abdomen, and include:
-
Feeling restless, wound-up, or on-edge
-
Being easily fatigued
-
Having difficulty concentrating; mind going blank
-
Being irritable
-
Having muscle tension
-
Difficulty controlling feelings of worry
-
Presence of ‘self-soothing’ behaviours such as nail-chewing or handrubbing
-
Having sleep problems, such as difficulty falling or staying asleep, restlessness, or unsatisfying sleep [2]

What are Anxiety Disorders?
Anxiety disorders are different from having occasional worries or fears. When you are experiencing an anxiety disorder, the anxiety does not go away and sometimes it continues to grow and keeps getting worse over time. Abnormal anxiety will interfere with daily activities, making work, relationships, and normal functioning difficult. [3]
There are five major types of anxiety disorders:
- Generalized Anxiety Disorder (GAD). The key signs of a GAD are chronic anxiety, worry and tension, even when there is no cause for anxiety and nothing is wrong.
- Panic Disorder. This type of anxiety disorder causes episodes of intense fear accompanied by physical symptoms including chest pain, heart palpitations, shortness of breath, dizziness, or abdominal distress. The panic episodes are unexpected and repeated.
- Social Anxiety Disorder. This is also known as Social Phobia. The key signs of this type of anxiety are overwhelming anxiety and excessive self-consciousness in normal daily social situations. In some cases, social phobia is limited to a specific situation, such as public speaking or having to eat and drink in front of other people. However it can also be so severe that symptoms are felt anytime other people are around.
- Obsessive-Compulsive Disorder (OCD). Symptoms of this form of anxiety are recurrent, unwanted thoughts (obsessions) and/or repetitive behaviors (compulsions). Common compulsions include hand washing, counting, checking, or cleaning and they are usually done in the hope of either preventing or ending the obsessive thoughts. If the ritual behaviours are not performed in the ‘correct’ sequence or at the ‘correct’ time the anxiety increases and often triggers more obsessive thinking. A recent review study found that women’s symptoms are somewhat different than men’s. Women exhibit more contamination and cleaning behaviours compared to men’s greater sexual-religious and aggressive symptoms. Women were also more likely to have eating and impulse-control disorders at the same time as the OCD. [3a]
- Post-Traumatic Stress Disorder (PTSD). This type of anxiety disorder may develop after exposure to a traumatic event or ordeal such as violent assaults, natural or human-caused disasters, accidents, or military combat, where grave physical harm did or could have occurred. [4]

Generalized Anxiety Disorder
The most common type of anxiety disorder that starts during the menopausal transition is generalized anxiety disorder (GAD). Be aware though that even if you have increased anxiety compared to your life before entering the menopausal transition, you may not meet the criteria for GAD.
The Diagnostic and Statistical Manual of Mental Disorders (DSM-5) is the standard classification of mental disorders used by health professionals in North America.[5] The DSM-5 outlines the following criterion to make a diagnosis of Generalized Anxiety Disorder:
- Excessive anxiety and worry (apprehensive expectation), occurring more days than not for at least 6 months, about a number of events or activities (such as work or school performance)
- The individual finds it difficult to control the worry.
- The anxiety and worry are associated with three (or more) of the following six symptoms (With at least some symptoms having been present for more days than not for the past 6 months).
- Restlessness or feeling keyed up or on edge.
- Being easily fatigued.
- Difficulty concentrating or mind going blank.
- Irritability.
- Muscle tension.
- Sleep disturbance (difficulty falling or staying asleep, or restless, unsatisfying sleep)
- The anxiety, worry, or physical symptoms cause clinically significant distress or impairment in social occupational, or other important areas of functioning.
- The disturbance is not attributable to the physiological effects of a substance (e.g., a drug of abuse, a medication) or another medical condition (e.g., hyperthyroidism).
- The disturbance is not better explained by another mental disorder (e.g., anxiety or worry about having panic attacks in panic disorder, a negative evaluation in social anxiety disorder, etc.
If you are concerned that you may be experiencing generalized anxiety disorder, use this brief scale called the GAD-7 to assess your anxiety symptoms. If you score with moderate or severe anxiety, please see your healthcare provider to discuss treatment and management. [6]

Panic Attacks vs Anxiety Attacks
Learn More
Panic Attacks vs Anxiety Attacks
Panic attacks can happen during the menopausal transition. Panic attacks come on suddenly, often with no warning, and typically last for 5 – 20 minutes. They may also occur in a series of episodes, one after another, for hours. [7] In some cases, hot flashes are accompanied by feelings that mimic or even trigger a panic attack. [8]
Symptoms of a panic attack include the following:
- rapid heart rate
- chest pain
- dizziness or lightheadedness
- hot flashes or chills
- nausea
- numbness or tingling in the extremities
- shaking
- shortness of breath
- stomach pain
- sweating.
During the panic attack itself, you may experience an overwhelming sense of losing control, sudden fear of dying, and a sense of being detached from the environment around you. Panic attacks are associated with a diagnosable panic disorder.
Anxiety attacks are often mistaken for a panic attack, but they differ in several important ways. Unlike panic attacks, an anxiety attack happens after a bout of intense and prolonged anxiety or worry. Symptoms are usually less intense than panic attack symptoms, although still scary. They are not part of a diagnosable disorder, but they do often happen as part of a generalized anxiety disorder (GAD). Symptoms of an anxiety attack overlap with the symptoms of GAD, as follows:
- nervousness
- irritability
- increased heart rate
- rapid breathing
- trembling
- sweating
- a sense of impending danger
- difficulty concentrating
- sleep disturbances
| Panic Attack | Anxiety Attack |
| Usually occurs after experiencing a trigger but can occur without one. | Usually occurs as a response to a perceived stressor or threat. |
| Symptoms appear suddenly. | Symptoms build gradually over time. |
| Symptoms are disruptive; you may feel detached from your surroundings. | Symptoms can vary in intensity from mild to severe. |
| Typically subside in minutes. | Symptoms may prevail for longer periods. |
[7]

Other Symptoms and Anxiety
Learn More
Other Menopausal Transition Symptoms and Anxiety
Vasomotor symptoms (hot flashes) and anxiety are consistently associated with each other in multiple studies. [9] Depression is also linked with both vasomotor symptoms and anxiety. It is unclear what the underlying factors are, but studies are continuing to explore this connection. [1]
The relationship between anxiety and depression is not totally clear, but researchers do know that about 85% of patients with depression will also experience symptoms of anxiety. And it works in both directions – about 90% of patients with anxiety disorders also experience depression. This overlap of symptoms from anxiety and depression makes research and treatment challenging. Anxiety and depression can also be experienced separately. [10]
Insomnia is another common symptom of the menopausal transition, with 40-50% of women experiencing it. Insomnia and difficulties sleeping are strongly associated with anxiety and depression. [7] One study looking at the relationship amongst anxiety, depression, and insomnia found that difficulty falling asleep is strongly associated with symptoms of anxiety, while the feeling that sleep was not refreshing or restorative is strongly correlated with depression.[11]
Self-care & Natural Remedies for
Anxiety
Self-care for anxiety starts with compassion and kindness for yourself. Anxiety is awful and you do not deserve it, nor did you ‘ask’ for it. It can just happen, regardless of whether it seems rational. There are things that you can do, however, to help make it through this challenging symptom.
- Talk to someone you trust. A problem shared is a problem halved, or so the saying goes. While talking to someone isn’t going to stop the worry (whether it is justified or not), having someone listening and hearing your concerns can be a huge relief. Sometimes just sharing your worries can provide some perspective and lessen the anxiety, even temporarily.
- Manage the anxiety. There are many different worries in all of our lives, some of which we can control and some of which we can’t. Regardless of the ability to control them, giving them dedicated time can be helpful. Set aside a specific time, even using a timer if it helps, to focus on what is worrying you. Acknowledging your anxiety without feeling guilty or shameful for worrying can be a huge help. You can also write down your worries or record them in a way that makes sense to you. When you find a specific time and method to address your worries, it can become easier to avoid worrying about them all the time and simply postpone them until your next ‘worry session’.
- Take care of your physical body. Your worries may not be specifically about your health, but it doesn’t matter. When you eat well, get adequate exercise, and have good quality sleep, you will feel better. Full stop. The worries may still be there, but they won’t feel as crushing.
- Practice meditation and/or breathing exercises. These practices help calm your mind and can reduce the strength of the anxiety. They are very helpful if you have menopause anxiety at night. Mindfulness, the practice of focusing your full attention on the present moment may help, but, in some cases mindfulness has been shown to make anxiety worse. This happens when your attention is on the present moment, which in this case means total focus on your worries. Be aware of this, and if you try a mindfulness practice, do not feel bad or shameful if it doesn’t work. Just let it go and try something else.
- Journal your thoughts and feelings. Not only is keeping a journal a proven way to self-reflect and practice self-care, your journal can also help you track your worries and anxieties. You may start to see patterns in your anxiety, and identify situations that trigger feelings of worry or fear. Take the time to journal things that are good as well! This can be a boost when you are feeling down – it is often easy to forget our successes and only focus on the problems.
- Join a support group or a peer group. Your healthcare provider can give you a recommendation for a support group or point you to specialty care organizations such as Anxiety Care groups. Do an internet search to find supportive groups near you. You may also find online groups that specialize in providing support for anxiety problems.
- Practice Mind Body Wellness therapies. Refer to the Herstasis therapy page Mind Body Wellness to explore options for alternative and complementary treatments that may help you. Yoga, biofeedback and relaxation therapy, hypnosis, aromatherapy, meditative movement such as Tai Chi or Qigong, are all described in detail, as are several others. You may get inspired to try one or more of these and see if it helps calm your anxiety. [12]
- Creating a safe physical space. When anxiety is high, one way to soothe yourself is to make a cozy and safe space for yourself. Try using a weighted blanket, or creating a warm ‘fort’ with blankets or pillows.
Therapy & Treatment for Anxiety
The good news is that anxiety can be helped. If you have had or are having anxiety, please ensure you have professional therapeutic care heading into perimenopause. At age 40 find a reliable, educated primary care provider familiar with recognizing and treating symptoms of perimenopause and menopause. The North American Menopause Society provides a list of menopause practitioners here.
Anxiety in women is very common across all ages starting in adolescence. The Women’s Preventive Services Initiative (WPSI), a national coalition of women’s health professional organizations and patient representatives in the US recommends screening for anxiety in women and adolescent girls aged 13 years or older who are not currently diagnosed with anxiety disorders, including pregnant and postpartum women. [13] Medications or therapy, either combined or separately, are the typical treatments for anxiety. [8]

Therapy and Counselling
Learn More
Therapy and Counselling
Cognitive behavioural therapy (CBT) is a type of psychotherapy based on the idea that your thought patterns affect your emotions, which can then affect your behaviors. CBT can teach people different ways of thinking, behaving, and reacting to situations to help reduce anxiety. For example, CBT recognizes that negative, worrying thoughts can lead to fearful, worrisome feelings and actions. Reframing your thoughts to be more positive can lead to more positive feelings and helpful behaviors.
With a therapist using CBT, you will:
- identify specific problems or issues in your daily life
- increase your awareness of negative thought patterns and how they can impact your life
- identify negative thinking and reframing it in a way that changes how you feel
- learn new behaviors and putting them into practice [13a]
Exposure therapy is a technique used in CBT that has patients confront the fears underlying their anxiety. This helps get individuals back doing activities that they have been avoiding due to anxiety. Relaxation techniques are used to help manage anxiety while doing the exposure therapy. [14]
Acceptance and commitment therapy (ACT) is another type of therapy that can be used specifically to treat anxiety. ACT teaches and uses strategies such as mindfulness to reduce anxiety. It is a newer form of therapy than CBT, so at this time, less information is available on its long-term effectiveness. [14]

Medication
Learn More
Medication
Anti-anxiety medications work specifically to reduce the symptoms of anxiety including panic attacks and extreme worry and fear. Benzodiazepines are the most common class of anti-anxiety medications. They are very effective in helping to reduce anxiety, and they start working more quickly than most antidepressant medications. Benzodiazepines are the first-line treatment for generalized anxiety disorder. Unfortunately, it is easy to build up tolerance to benzodiazepines and start requiring higher and higher dosages to get the same calming effect. It is possible to become dependent on them and to experience withdrawal symptoms when the medication is stopped. Because of this, your health care provider will probably only prescribe benzodiazepines for a short period of time. If you are on benzodiazepines, your healthcare provider can work with you to safely decrease your dosages when you are ready to stop using them. [14]
Antidepressants are helpful to treat anxiety as well as depression. Anxiety is closely linked to the neurotransmitter molecule serotonin. Taking Selective Serotonin Reuptake Inhibitors (SSRIs) can help anxiety by working to maintain high circulating levels of serotonin in the blood. The Science section provides more detail on serotonin, and how it works to help in the treatment of anxiety. [14]
Beta-blockers are a medication usually used to treat high blood pressure. They are very useful to help relieve the physical symptoms of anxiety, including rapid heartbeat and shaking or trembling. They can also be used on an as-needed basis to help with episodes of acute anxiety, including some predictable forms of social anxiety such as public speaking or performing. [14]
The Science
Hormones and Neurotransmitters
Hormones and neurotransmitters are both chemical signaling molecules produced in our bodies. The primary difference between hormones and neurotransmitters is that hormones are produced in endocrine glands and are released into the bloodstream where they travel away from their place of origin to act on a target.
Neurotransmitters, on the other hand, enable nerve impulses to travel between neurons, or nerve cells.

Neurons
Neurons are the basic unit of the brain and nervous system, and they are responsible for sending and receiving signals from your brain throughout your body. For example, when neurons receive the sensory input of heat from cells in your hand, they transmit that information to the brain. Your brain, in turn, sends a signal back down through your neurons to the muscles in your arm, causing you to pull your hand away from the hot stove.

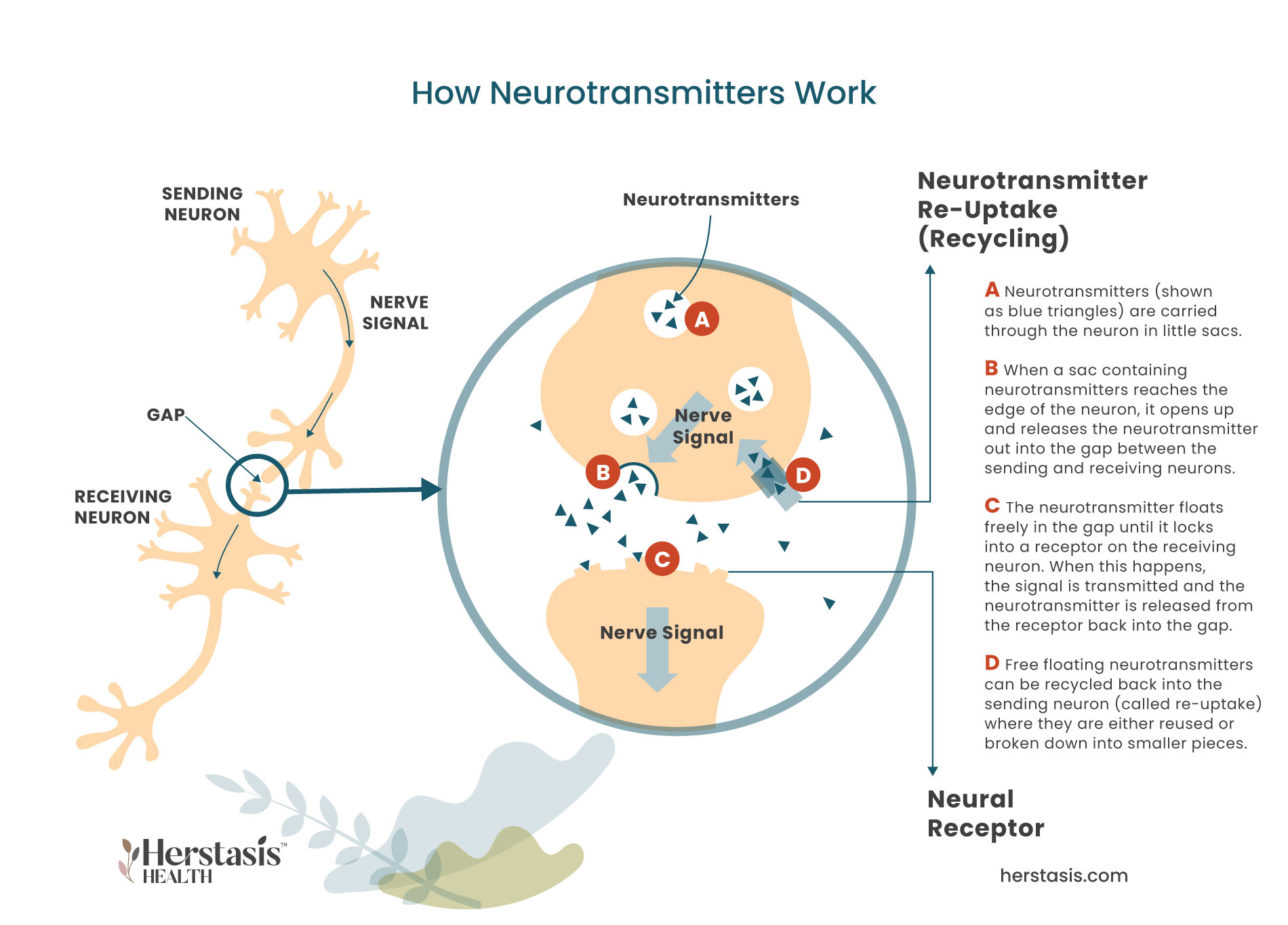
Nerve Signals
Nerve signals, like the ones in the diagram to the left, are passed from the sending neuron via neurotransmitters (A) that bridge the gap between neurons where they attach to receptors in the receiving neuron (B). When the neurotransmitter lands in the neural receptor on the receiving neuron, the nerve signal has been transmitted (C). The neurotransmitter is released from the receptor back into the gap where it will be broken down and destroyed by enzymes. Alternatively, it can be returned back into the sending neuron where it will be reused or it will be broken down into its component parts until they are needed again (D). Nerve signals travel this way through millions of nerve cells until the signal reaches its destination. There are about 60 km (or 37 miles) of nerve cells stretched end to end throughout the human body!
Depression and anxiety are closely linked to the neurotransmitter molecule serotonin, which is nicknamed the ‘happiness molecule’ because it promotes feelings of well-being. While serotonin is a neurotransmitter, it can also function like a hormone, allowing it to have effects outside of the central nervous system. For example, serotonin has been shown to help with, among others, regulating appetite and temperature, maintaining energy balance, bone remodeling, and sleep cycles. [13]
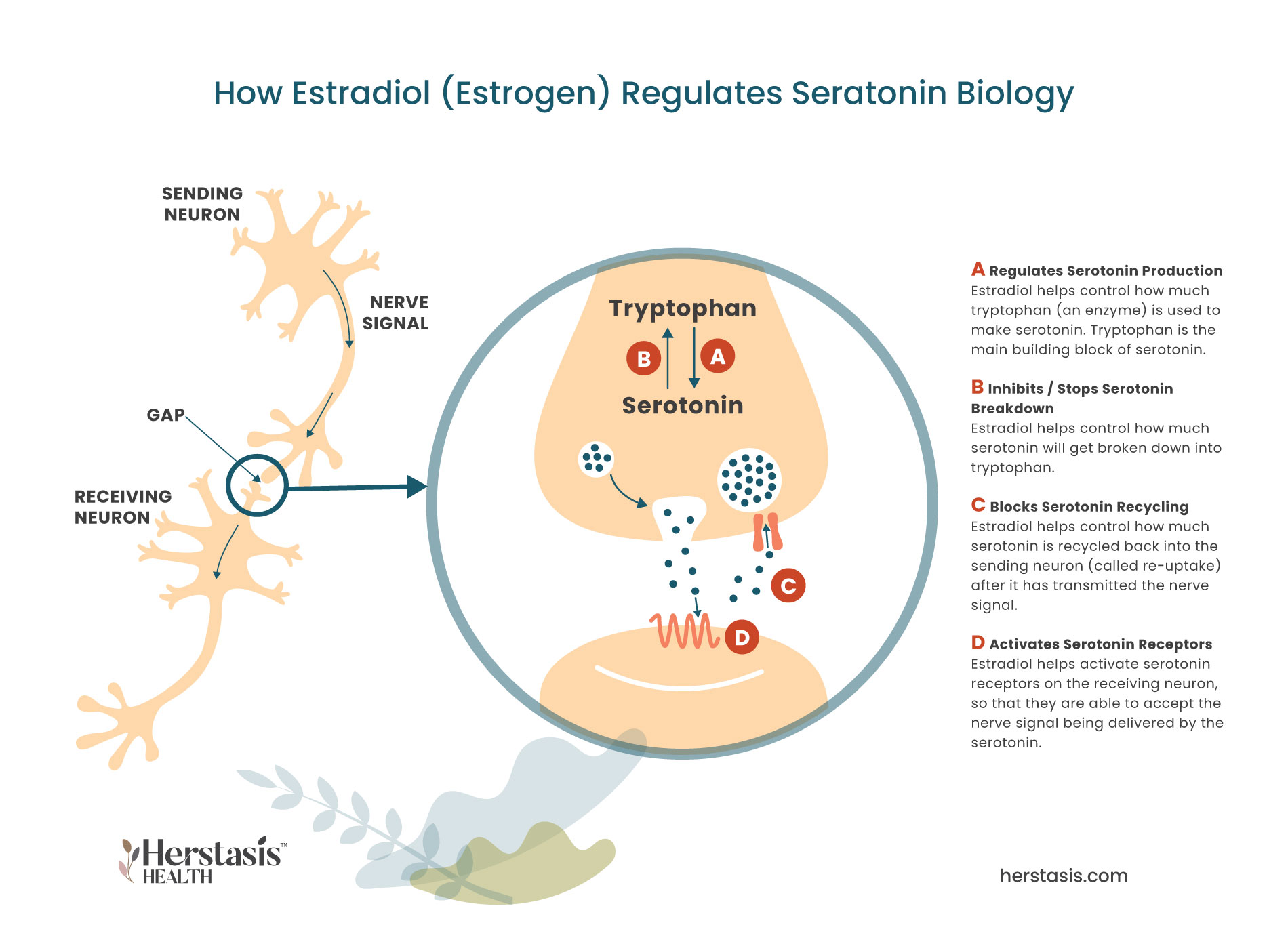
Serotonin communicates with other molecules in order to perform its many roles, so hormones, particularly the female hormone estradiol (a form of estrogen), play a very important role in managing serotonin signaling. [14] For example, estradiol has been shown to be involved in, although not necessarily causing, pain transmission, headaches, dizziness, nausea, and depression, all of which occur as a result of some level of serotonin activity. [2] As well, estrogen increases serotonin receptor density in select brain regions including the hypothalamus. [1] In fact, estradiol directly modulates just about everything about serotonin biology (see the diagram below), so anxiety and low estrogen commonly go together. Ways in which estradiol impacts serotonin include:
- regulating the expression of the enzyme (named tryptophan hydroxylase) that is required to build serotonin;
- helping activate serotonin receptor activity in the receiving neurons;
- blocking serotonin re-uptake (recycling) in the sending neuron by suppressing the enzyme (named monoamine oxidase) that breaks down serotonin into its inactive form. [15]

During the menopausal transition
During the menopausal transition, when estradiol levels start to drop, the levels of the enzyme tryptophan hydroxylase drops. This enzyme is the first ingredient needed to make serotonin, so when it becomes less available, less serotonin is being produced. In addition, serotonin production is further reduced because the expression of a different enzyme, monoamine oxidase, is no longer suppressed. This means that any free available serotonin is targeted by this enzyme and as a result, it gets rapidly broken down and becomes inactive. [6]

Neurobiologically
Neurobiologically, both vasomotor symptoms and depression are partially regulated by neurotransmitters, including serotonin. When these neurotransmitter systems become imbalanced and stop functioning properly, it can lead to depression if the imbalance occurs inside neural circuits (located in the brain) that are involved in mood regulation. However, when the imbalance occurs within the neural circuits involved in thermoregulation (temperature control) it can lead to vasomotor symptoms . [6]

Low serotonin levels add to menopausal transition symptoms
Low serotonin levels add to menopausal transition symptoms such as insomnia, hot flashes, depression and brain fog. Because of this, some women’s symptoms will be helped by taking Selective Serotonin Reuptake Inhibitors (SSRIs), which are a type of antidepressant. SSRIs can work for menopausal transition symptoms because they block serotonin from being recycled back into the sending neuron – a process called reuptake. This results in having more serotonin available to transmit nerve signals from neuron to neuron. Having more serotonin working helps lessen the severity of hot flashes or mood swings because the lower the serotonin levels, the stronger the symptoms. [6]
MYTH
It is true that antidepressants are used as a long-term treatment option for some people diagnosed with anxiety. Psychotherapy, which is often prescribed along with antidepressants, can help you learn strategies to cope with any anxiety you are facing. As you get more skilled at coping, it is possible to wean yourself off of antidepressants used for treating anxiety.
MYTH
Anxiety is a real and serious medical condition. It is not a choice, nor is it a sign of weakness. It will not be resolved by thinking calm, relaxed thoughts alone. Changing your attitude can be helpful as part of a suite of interventions, but on its own, it is unlikely to resolve anxiety in the long-term. It is KEY to seek professional help.
YES
In time the anxiety will go away on its own, although you may continue to experience bouts of anxiety if you have worries in your life. Menopause anxiety is caused by the changes in your hormone levels as you enter into the menopausal transition. When your hormone levels stabilize after reaching menopause (when you haven’t had a period for one full year / 12 months) your anxiety should also stabilize and go away.
Anxiety is unpleasant regardless of why it starts. Anxiety is characterized by feelings of worry, feeling restless and on-edge, having difficulty focusing, and being irritable. It is also common to have insomnia, feel physically tense, and experience fatigue. Anxiety that starts during the menopausal transition is usually generalized anxiety, and you will feel chronic anxiety, worry and tension, even when there is no cause for anxiety and nothing is wrong. If you are already experiencing an anxiety disorder, such as social anxiety or obsessive compulsive disorder, your symptoms may get worse. See your healthcare provider to find the best treatment(s) to manage your anxiety.
Anxiety is anxiety, regardless of whether menopause triggers it, so symptoms of menopause anxiety are the same as those felt with non-menopause anxiety. Symptoms associated with anxiety are commonly felt in the chest or abdomen, and include:
- Feeling restless, wound-up, or on-edge
- Being easily fatigued
- Having difficulty concentrating; mind going blank
- Being irritable
- Having muscle tension
- Difficulty controlling feelings of worry
- Presence of ‘self-soothing’ behaviours such as nail-chewing or handrubbing
- Having sleep problems, such as difficulty falling or staying asleep, restlessness, or unsatisfying sleep [2]
Anxiety that starts during the menopausal transition will typically resolve itself once your hormones stabilize as you enter menopause. It is still important to seek help if your anxiety is strong because anxiety is treatable. There is no need to suffer for the length of your menopausal transition.
MYTH
Stress is part of life and can be very hard, if not impossible, to avoid. It is important to seek out help to learn effective coping strategies for stressful situations. This is especially important if you are aware that certain situations (like interpersonal conflict) can trigger your anxiety. Finding coping strategies that work is possible and using them successfully can have broader positive impacts as you successfully manage stressful situations.
YES
Anxiety is not just feeling worried and it is not a character flaw. They are complex disorders that have social, psychological and biological causes. Do not think that you can just think them away, or that they are normal. Help is available so talk to your healthcare provider. While sadness, stress, anxiety, and worry are normal and common, when they occur frequently and/or in intense episodes, this is a real and serious medical problem.
Compiled References
[1] Jaeger MB, Miná CS, Alves S, Schuh GJ, Wender MC, Manfro GG. Negative affect symptoms, anxiety sensitivity, and vasomotor symptoms during perimenopause. Braz J Psychiatry. 2021 May-Jun;43(3):277-284. doi: 10.1590/1516-4446-2020-0871. PMID: 33053044; PMCID: PMC8136388.
[2] https://www.nimh.nih.gov/health/topics/anxiety-disorders
[3] https://www.nimh.nih.gov/health/topics/anxiety-disorders
[3a] Mathis MA, Alvarenga Pd, Funaro G, Torresan RC, Moraes I, Torres AR, Zilberman ML, Hounie AG. Gender differences in obsessive-compulsive disorder: a literature review. Braz J Psychiatry. 2011 Dec;33(4):390-9. doi: 10.1590/s1516-44462011000400014. PMID: 22189930.
[5] American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596
[6] https://adaa.org/sites/default/files/GAD-7_Anxiety-updated_0.pdf
[7] https://www.medicalnewstoday.com/articles/317552#anxiety-and-menopause
[8] https://www.menopause.org/for-women/menopauseflashes/menopause-symptoms-and-treatments/going-mad-in-perimenopause-signs-and-solutions
[9] Thurston RC, Joffe H. Vasomotor symptoms and menopause: findings from the Study of Women’s Health across the Nation. Obstet Gynecol Clin North Am. 2011 Sep;38(3):489-501. doi: 10.1016/j.ogc.2011.05.006. PMID: 21961716; PMCID: PMC3185243.
[10] Gorman JM. Comorbid depression and anxiety spectrum disorders. Depress Anxiety. 1996-1997;4(4):160-8. doi: 10.1002/(SICI)1520-6394(1996)4:4<160::AID-DA2>3.0.CO;2-J. PMID: 9166648.
[11] Masakazu Terauchi,Shiro Hiramitsu, Mihoko Akiyoshi Yoko Owa, Kiyoko Kato
Satoshi Obayashi,Eisuke Matsushima,Toshiro Kubota (2012) Associations between anxiety, depression and insomnia in peri- and post-menopausal women. Maturitas Volume 72, Issue 1, pg 61-65.:https://doi.org/10.1016/j.maturitas.2012.01.014
[13] https://www.womenspreventivehealth.org/recommendations/screening-for-anxiety/
[13a] https://www.healthline.com/health/cbt-techniques
[14] https://www.nimh.nih.gov/health/topics/anxiety-disorders#part_2225
[15] https://www.zrtlab.com/blog/archive/impact-hormones-serotonin-depression/#_edn12
[16] Rybaczyk LA, Bashaw MJ, Pathak DR, Moody SM, Gilders RM, Holzschu DL. An overlooked connection: serotonergic mediation of estrogen-related physiology and pathology. BMC Womens Health. 2005;5:12. Published 2005 Dec 20. doi:10.1186/1472-6874-5-12
[17] Parry, Barbara L. MD Towards improving recognition and management of perimenopausal depression, Menopause: April 2020 – Volume 27 – Issue 4 – p 377-379
doi: 10.1097/GME.0000000000001519
[18] Maki, Pauline M. PhD1; Freeman, Ellen W. PhD2; Greendale, Gail A. MD3; Henderson, Victor W. MD, MS4; Newhouse, Paul A. MD5; Schmidt, Peter J. MD6; Scott, Nelda F. MD7; Shively, Carol A. PhD8; Soares, Claudio N. MD, PhD, FRCP9 Summary of the National Institute on Aging-sponsored conference on depressive symptoms and cognitive complaints in the menopausal transition, Menopause: July 2010 – Volume 17 – Issue 4 – p 815-822
doi: 10.1097/gme.0b013e3181d763d2
[19] https://www.zrtlab.com/blog/archive/mood-menopause-perimenopause
[20] Wise, D., Felker, A., & Stahl, S. (2008). Tailoring Treatment of Depression for Women Across the Reproductive Lifecycle: The Importance of Pregnancy, Vasomotor Symptoms, and Other Estrogen-Related Events in Psychopharmacology. CNS Spectrums, 13(8), 647-662. doi:10.1017/S1092852900013742