What are anxiety and depression?
Sadness is the hallmark symptom of depression. It is a normal emotion and can be experienced regularly, especially during times of change and/or stress. However, when sadness is persistent, creates challenges to daily functioning, or is seen at the same time as other physical and cognitive symptoms, it requires intervention. Even “minor” depression-states that do not meet diagnostic criteria for a major depressive episode (see below) can cause significant impairment in daily life. [1][2]

Classifying Anxiety & Depression

Even “minor” depression-states that do not meet diagnostic criteria for a major depressive episode (see below) can cause significant impairment in daily life. [1]
The Diagnostic and Statistical Manual of Mental Disorders (DSM-5) is the standard classification of mental disorders used by health professionals in North America.[3] The DSM-5 outlines the following criterion to make a diagnosis of depression:
The individual must be experiencing five or more symptoms during the same 2-week period and at least one of the symptoms should be either (1) depressed mood or (2) loss of interest or pleasure.
- Depressed mood most of the day, nearly every day.
- Markedly diminished interest or pleasure in all, or almost all, activities most of the day, nearly every day.
- Significant weight loss when not dieting or weight gain, or decrease or increase in appetite nearly every day.
- A slowing down of thought and a reduction of physical movement (observable by others, not merely subjective feelings of restlessness or being slowed down).
- Fatigue or loss of energy nearly every day.
- Feelings of worthlessness or excessive or inappropriate guilt nearly every day.
- Diminished ability to think or concentrate, or indecisiveness, nearly every day.
- Recurrent thoughts of death, recurrent suicidal ideation* without a specific plan, or a suicide attempt or a specific plan for committing suicide.
If you or someone you know are experiencing suicide ideation, PLEASE read out for help. These resources can help you.
It CAN and WILL get better.
*also known as suicidal thoughts or ideas. This term describes a range of thinking, wishing, and preoccupation with death and suicide.

Symptoms of Depression & Anxiety
The relationship between anxiety and depression is not totally clear, but researchers do know that about 85% of patients with depression will also experience symptoms of anxiety. And it works in both directions – about 90% of patients with anxiety disorders also experience depression. This overlap of symptoms from anxiety and depression makes research and treatment challenging. Anxiety and depression can also be experienced separately. [4]
Symptoms associated with anxiety and commonly felt in the chest or solar plexus include: [5]
- Feeling restless, wound-up, or on-edge
- Being easily fatigued
- Having difficulty concentrating; mind going blank
- Being irritable
- Having muscle tension
- Difficulty controlling feelings of worry
- Having sleep problems, such as difficulty falling or staying asleep, restlessness, or unsatisfying sleep
Depression and anxiety are serious, potentially life-threatening symptoms. They are not the symptoms you decide to just ‘push through’, especially because they can be successfully treated. Immediately talk to your doctor if you have a history of depression and your previous symptoms return or if you have new symptoms even without a history of depression.
The menopausal transition and early postmenopausal period are associated with an increased risk for clinically significant depressive symptoms.[6] [7] Women with no history of major depression are two to four times more likely to report depressed mood in the menopausal transition compared with the premenopausal stage. [1] Women with a history of anxiety and depression, including postpartum depression, are also at higher risk to experience these symptoms during the menopausal transition.
Resources:

Hormones and Anxiety & Depression
Changes in hormone levels during the menopausal transition are thought to contribute to depression. This has been shown in studies looking at associations between depression, menopausal stage, variability in estradiol (estrogen) levels, and increasing follicle-stimulating hormone (FSH) levels. Other risk factors for depression include poor sleep, hot flashes, stressful or negative life events, lack of employment, age, and race. As well, chronic stress of any kind can contribute to anxiety and depression, and in turn, anxiety and depression can make chronic stress worse. [1]
Vasomotor symptoms and depression are linked. Perimenopausal women with vasomotor symptoms are four times more likely to be depressed than perimenopausal women without vasomotor symptoms. This risk lowers after menopause at the same time that vasomotor symptoms also seem to subside, supporting the hypothesis that that risk for depression and for vasomotor symptoms are correlated with fluctuations in hormone levels – as you would see during the tumultuous perimenopausal stage – rather than with absolute levels of hormones. [6]
Insomnia and depression are also linked. Poor sleep can make you up to 10 times more likely to become depressed. [8] One research study looked at the correlation between physical and psychological symptoms and insomnia, and also at the contribution of depression and anxiety to insomnia. The results showed that insomnia is very common among peri- and post-menopausal female patients in a clinical setting, and that insomnia is more closely associated with psychological symptoms such as anxiety or depression than with physical symptoms. Interestingly, the study found that difficulty falling asleep is strongly associated with symptoms of anxiety while non-restorative sleep (NRS) – or the feeling that sleep was not refreshing or restorative – is strongly correlated with depression.[9]
Self-care for anxiety and depression
Self-care for anxiety and depression starts with compassion for yourself. Depression and anxiety are not something that you asked for, or that you deserve. They just happen, regardless of “how happy you should be”. There are things that you can do, however, to help make it through these challenging symptoms.
You can support yourself with meditation, journaling, finding calm and peace outdoors in nature and by engaging your creative side through art and music. Try to choose a healthy lifestyle when you can, with enough quality sleep, good nutrition and recreational exercise. Cut down on alcohol, recreational drugs, and late nights. Track emotional events carefully on a daily basis. Look for patterns and triggers such as certain people, events, activities and even foods.
There is no shame in experiencing depression and anxiety, despite the historical bias about acknowledging mental health symptoms.
Talk. Talk to your girlfriends about menopause. Talk with your family about what you are experiencing. Talk to your employer and ask for support and compassion. You will probably be surprised to find how many others have been suffering in silence, just waiting for someone else (you!) to have enough courage to start the conversation.
YOU ARE NOT ALONE.
You are entitled to support and compassion from others. Advocate for yourself, and remember, mental health challenges are as valid as physical health challenges.
It is very important to seek professional help. Anxiety and depression are awful to experience, but they can also be very dangerous. Individual therapy and counseling can provide you with tools for recognizing and working through these common symptoms of perimenopause.
Research has shown that women who make more positive adjustments (both physical and mental) to manage the menopausal transition experience less severe stress, psychological distress, fewer menopause symptoms, and better physical health. These results suggest that women who expect menopause to be a negative experience or are highly stressed or distressed may be more likely to experience a more negative menopause. [10] While it may not be easy to shift your mindset, some therapies such as cognitive behavioural therapy (CBT) may be very helpful. CBT is discussed in more detail in the following section – Therapy for Anxiety and Depression.

Therapy for anxiety and depression
The good news is that depression and anxiety can be helped. If you have had or are having either (or both) anxiety and depression, please ensure you have professional therapeutic care heading into perimenopause. At age 40 find a reliable, educated primary care provider familiar with recognizing and treating symptoms of perimenopause and menopause. The North American Menopause Society provides a list of menopause practitioners here.
It is very important to understand that not all healthcare providers regularly screen for depression in perimenopausal women [2], so you may need to advocate for yourself if you are concerned about any depressive or anxious symptoms. You can request that your healthcare provider use the Patient Health Questionnaire (PHQ-9), which is a tool designed to screen for depression. You can also access this self-report questionnaire yourself online or in our resources section, so you can fill it out and tell your healthcare provider the results.
Your healthcare providers and therapists may ask you to try medications tailored to your specific mental health needs. Many women respond well to Hormone Therapy (HT). Hormone therapy (HT) with estrogen, which is safe and often effective for reducing hot flashes and night sweats . This may help improve sleep quality, and these improvements in your sleep may help regulate anxiety and depression.
One randomized trial demonstrated that the transdermal estradiol patch (one type of estrogen HT) given for 12 weeks was very useful for treating depression in perimenopausal women, with remission rates as high as 60% to 80%. [12] A different study found that the same transdermal estradiol did not have an antidepressant effect when given to postmenopausal women, after they completed the menopausal transition. If the results of these two studies are taken together, they show that the menopausal transition is a ‘window of opportunity’ to use estrogen-based strategies for the management of depression.[1]
Your healthcare provider may prescribe antidepressants that can be helpful to treat anxiety and depression in women who are not candidates for hormone therapy. The Science section below provides more detail on the types of antidepressants that may be most beneficial, as well as why they may be helpful. If your depression is deep, treatment may require antidepressants plus cognitive behavioural therapy, as studies have shown that this is the most effective combination to treat depression.
Cognitive behavioural therapy (CBT) is based on the idea that your thought patterns affect your emotions, which can then affect your behaviors. For example, CBT recognizes that negative thoughts can lead to negative feelings and actions. Reframing your thoughts to be more positive can lead to more positive feelings and helpful behaviors. CBT typically includes:
- identifying specific problems or issues in your daily life;
- increasing your awareness of negative thought patterns and how they can impact your life;
- identifying negative thinking and reframing it in a way that changes how you feel; and
- learning new behaviors and putting them into practice [11]
New research is being conducted on the prevention of depression and anxiety. One study looked at using hormone therapy to prevent the onset of perimenopausal and early postmenopausal depressive symptoms – not just to treat it once it has occurred. The results from a randomized clinical trial showed that hormone therapy treatment with transdermal estradiol plus intermittent micronized progesterone (TE+IMP) can be effective in preventing the development of clinically significant depressive symptoms. A twelve month course of TE+IMP was more effective than placebo in preventing the development of clinically significant depressive symptoms among initially emotionally stable perimenopausal and early postmenopausal women. [7]
The Science
Hormones and Neurotransmitters
Hormones and neurotransmitters are both chemical signaling molecules produced in our bodies. The primary difference between hormones and neurotransmitters is that hormones are produced in endocrine glands and are released into the bloodstream where they travel away from their place of origin to act on a target.
Neurotransmitters, on the other hand, enable nerve impulses to travel between neurons, or nerve cells.

Neurons
Neurons are the basic unit of the brain and nervous system, and they are responsible for sending and receiving signals from your brain throughout your body. For example, when neurons receive the sensory input of heat from cells in your hand, they transmit that information to the brain. Your brain, in turn, sends a signal back down through your neurons to the muscles in your arm, causing you to pull your hand away from the hot stove.

Nerve Signals
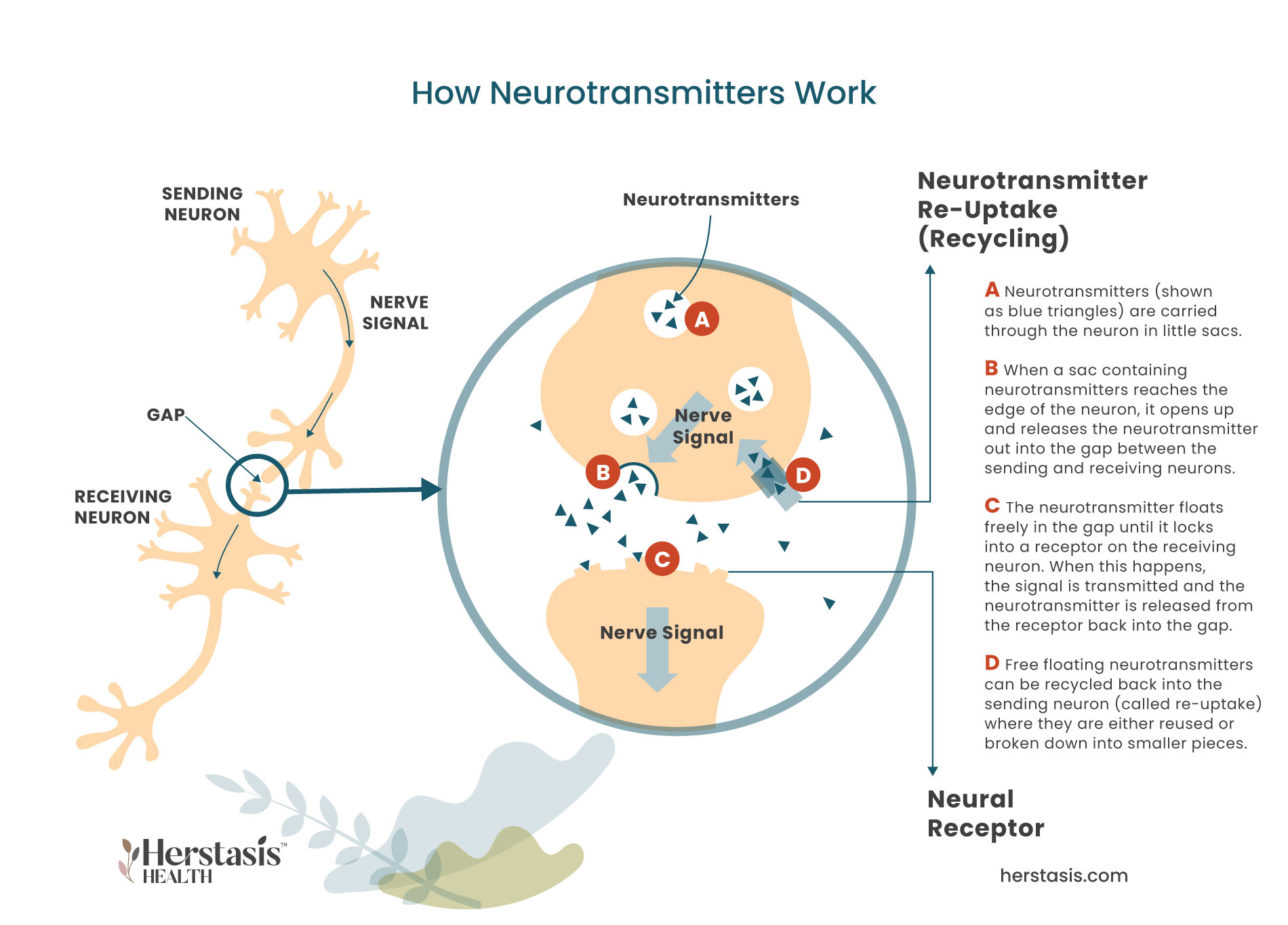
Nerve signals, like the ones in the diagram to the left, are passed from the sending neuron via neurotransmitters (A) that bridge the gap between neurons where they attach to receptors in the receiving neuron (B). When the neurotransmitter lands in the neural receptor on the receiving neuron, the nerve signal has been transmitted (C). The neurotransmitter is released from the receptor back into the gap where it will be broken down and destroyed by enzymes. Alternatively, it can be returned back into the sending neuron where it will be reused or it will be broken down into its component parts until they are needed again (D). Nerve signals travel this way through millions of nerve cells until the signal reaches its destination. There are about 60 km (or 37 miles) of nerve cells stretched end to end throughout the human body!
Depression and anxiety are closely linked to the neurotransmitter molecule serotonin, which is nicknamed the ‘happiness molecule’ because it promotes feelings of well-being. While serotonin is a neurotransmitter, it can also function like a hormone, allowing it to have effects outside of the central nervous system. For example, serotonin has been shown to help with, among others, regulating appetite and temperature, maintaining energy balance, bone remodeling, and sleep cycles. [13]
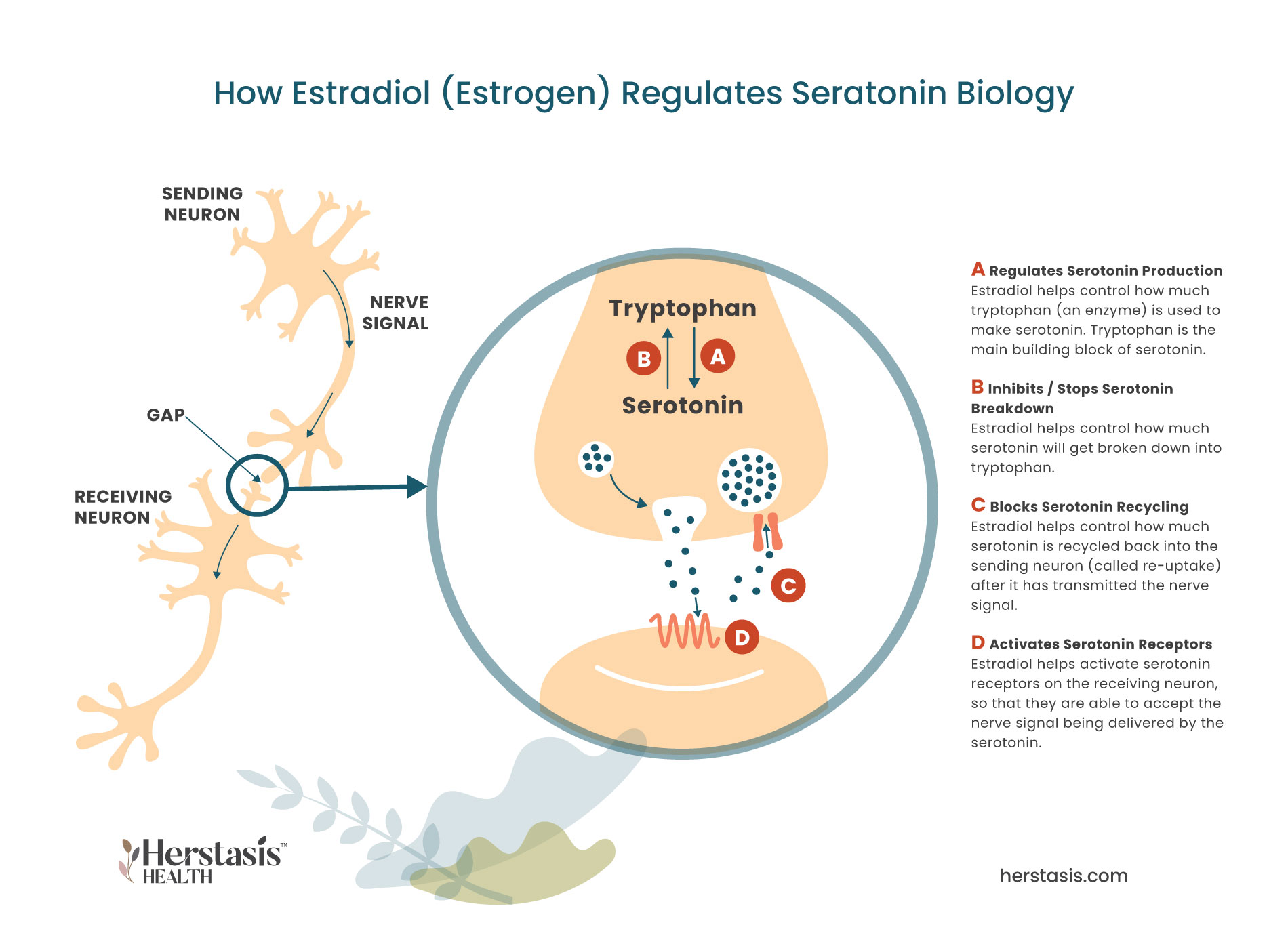
Serotonin communicates with other molecules in order to perform its many roles, so hormones, particularly the female hormone estradiol (a form of estrogen), play a very important role in managing serotonin signaling. [14] For example, estradiol has been shown to be involved in, although not necessarily causing, pain transmission, headaches, dizziness, nausea, and depression, all of which occur as a result of some level of serotonin activity. [2] As well, estrogen increases serotonin receptor density in select brain regions including the hypothalamus. [1] In fact, estradiol directly modulates just about everything about serotonin biology (see the diagram below), including:
- regulating the expression of the enzyme (named tryptophan hydroxylase) that is required to build serotonin;
- helping activate serotonin receptor activity in the receiving neurons;
- blocking serotonin re-uptake (recycling) in the sending neuron by suppressing the enzyme (named monoamine oxidase) that breaks down serotonin into its inactive form. [15]

During the menopausal transition
During the menopausal transition, when estradiol levels start to drop, the levels of the enzyme tryptophan hydroxylase drops. This enzyme is the first ingredient needed to make serotonin, so when it becomes less available, less serotonin is being produced. In addition, serotonin production is further reduced because the expression of a different enzyme, monoamine oxidase, is no longer suppressed. This means that any free available serotonin is targeted by this enzyme and as a result, it gets rapidly broken down and becomes inactive. [6]

Neurobiologically
Neurobiologically, both vasomotor symptoms and depression are partially regulated by neurotransmitters, including serotonin. When these neurotransmitter systems become imbalanced and stop functioning properly, it can lead to depression if the imbalance occurs inside neural circuits (located in the brain) that are involved in mood regulation. However, when the imbalance occurs within the neural circuits involved in thermoregulation (temperature control) it can lead to vasomotor symptoms . [6]

Low serotonin levels add to menopausal transition symptoms
Low serotonin levels add to menopausal transition symptoms such as insomnia, hot flashes, depression and brain fog. Because of this, some women’s symptoms will be helped by taking Selective Serotonin Reuptake Inhibitors (SSRIs), which are a type of antidepressant. SSRIs can work for menopausal transition symptoms because they block serotonin from being recycled back into the sending neuron – a process called reuptake. This results in having more serotonin available to transmit nerve signals from neuron to neuron. Having more serotonin working helps lessen the severity of hot flashes or mood swings because the lower the serotonin levels, the stronger the symptoms. [6]
MYTH
Unfortunately, many individuals suffering from depression have learned how to keep their symptoms secret, often out of fear or shame of being labeled with a mental health condition. Depression is so common in our society that it is very likely you know at least one, if not more, individuals that are suffering. If you aren’t sure, ask. It can be hard for those who are suffering to talk openly about their struggles.
MYTH
Discussing depression does not make it worse or keep you focused on feeling depressed. In fact, feeling isolated and alone in your depression can be very harmful and can make your depression worse. Talking to any supportive listener, be they a friend, family-member, or colleague, can be a huge help, especially if they have had or are having similar experiences. This can reinforce that you are not an awful or weak person, rather you are just struggling at the moment with a health crisis. Talking to a qualified and certified therapist or counselor can literally be a life-saver.
It is true that antidepressants are used as a long-term treatment option for some people diagnosed with depression. Psychotherapy, which is often prescribed along with antidepressants, can help you learn strategies to cope with the challenges you are facing. As you get more skilled at coping, it is possible to wean yourself off of antidepressants with medical supervision. However, if your depression is a result of imbalances in your brain chemistry, you may keep taking antidepressants indefinitely.
Consider that this is similar to taking high blood pressure medications. If you can control your high blood pressure with lifestyle adjustments then you may not need long-term medications for blood pressure management. If, however, your high blood pressure is caused by genetic or biological factors, you may need to stay on a long-term course of medication.
MYTH
Genetics do play a role and a family history of depression does increase the likelihood of experiencing depression. However, genetics is not the only factor at play, and everyone, regardless of family history, can work to minimize their risk of depression with simple actions like ensuring high quality sleep, eating nutritious food, exercising, and avoiding drugs and alcohol.
MYTH
Depression is a real and serious medical condition. It is not a choice or a sign of weakness. It will not be resolved by thinking happy thoughts alone. Changing your attitude can be helpful as part of a suite of interventions, but on its own, it is unlikely to resolve depression in the long-term. It is KEY to communicate how you feel to others and seek professional help.
MYTH
Depression is generally treatable, and antidepressants are a common tool that is used for treatment. However, antidepressants work by changing the chemistry in your brain, so they will not help if the cause of your depression is not biologically based, and they often take weeks if not months to take effect. In some cases, multiple antidepressants must be tried before the one that works for you and your brain chemistry is found. Many healthcare providers will also prescribe psychotherapy in addition to antidepressants.
MYTH
Depression is NOT just feeling sad and is not a character flaw Depression is a complex disorder that can have social, psychological and biological causes. Do not think that you can just wish it away, or that it is normal to feel this low all the time. While human sadness is part of our condition, when it occurs frequently and/or in intense episodes, this is a real and serious medical problem. Talk to your healthcare provider about how you feel.
Depression has complex root causes and can happen to any person, old or young, rich or poor, large and small. From the outside, you may seem to have “all you should need” and still be depressed. You may also have seemingly little, and have a high quality of life with balanced moods.
NO
Depression is NOT just feeling sad and is not a character flaw. Depression is a complex disorder that can have social, psychological and biological causes. Do not think that you can just wish it away, or that it is normal to feel this low all the time. While human sadness is part of our condition, when it occurs frequently and/or in intense episodes, this is a real and serious medical problem. Talk to your healthcare provider about how you feel.
FALSE
Discussing depression does not make it worse or keep you focused on feeling depressed. In fact, feeling isolated and alone in your depression can be very harmful and can make your depression worse. Talking to any supportive listener, be they a friend, family-member, or colleague, can be a huge help, especially if they have had or are having similar experiences. This can reinforce that you are not an awful or weak person, rather you are just struggling at the moment with a health crisis. Talking to a qualified and certified therapist or counselor can literally be a life-saver.
FALSE
It is true that antidepressants are used as a long-term treatment option for some people diagnosed with depression. Psychotherapy, which is often prescribed along with antidepressants, can help you learn strategies to cope with any challenges you are facing. As you get more skilled at coping, it is possible to wean yourself off of antidepressants. However, if your depression is a result of imbalances in your brain chemistry, you may keep taking antidepressants indefinitely. Consider that this is similar to taking high blood pressure medications. If you can control your high blood pressure with lifestyle adjustments then you may not need long-term medications for blood pressure management. If, however, your high blood pressure is caused by genetic or biological factors, you may need to stay on a long-term course of medication.
FALSE
Genetics do play a role and a family history of depression does increase the likelihood of experiencing depression. However, genetics is not the only factor at play, and everyone, regardless of family history, can work to minimize their risk of depression with simple actions like ensuring high quality sleep and avoiding drugs and alcohol.
FALSE
Depression is a real and serious medical condition. It is not a choice, nor is it a sign of weakness. It will not be resolved by thinking happy thoughts alone. Changing your attitude can be helpful as part of a suite of interventions, but on its own, it is unlikely to resolve depression in the long-term. It is KEY to seek professional help.
MYTH
Depression is generally treatable, and antidepressants are a common tool that is used for treatment. However, antidepressants work by changing the chemistry in your brain, so they will not help if the cause of your depression is not biologically based, and they often take weeks if not months to take effect. In some cases, multiple antidepressants must be tried before the one that works for you and your brain chemistry is found. Many healthcare providers will also prescribe psychotherapy in addition to antidepressants.
Compiled References
[1] Maki, Pauline M. PhD1; Freeman, Ellen W. PhD2; Greendale, Gail A. MD3; Henderson, Victor W. MD, MS4; Newhouse, Paul A. MD5; Schmidt, Peter J. MD6; Scott, Nelda F. MD7; Shively, Carol A. PhD8; Soares, Claudio N. MD, PhD, FRCP9 Summary of the National Institute on Aging-sponsored conference on depressive symptoms and cognitive complaints in the menopausal transition, Menopause: July 2010 – Volume 17 – Issue 4 – p 815-822
doi: 10.1097/gme.0b013e3181d763d2
[2] Parry, Barbara L. MD Towards improving recognition and management of perimenopausal depression, Menopause: April 2020 – Volume 27 – Issue 4 – p 377-379
doi: 10.1097/GME.0000000000001519
[3] American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596
[4] Gorman JM. Comorbid depression and anxiety spectrum disorders. Depress Anxiety. 1996-1997;4(4):160-8. doi: 10.1002/(SICI)1520-6394(1996)4:4<160::AID-DA2>3.0.CO;2-J. PMID: 9166648.
[5] https://www.nimh.nih.gov/health/topics/anxiety-disorders
[6] Wise, D., Felker, A., & Stahl, S. (2008). Tailoring Treatment of Depression for Women Across the Reproductive Lifecycle: The Importance of Pregnancy, Vasomotor Symptoms, and Other Estrogen-Related Events in Psychopharmacology. CNS Spectrums, 13(8), 647-662. doi:10.1017/S1092852900013742
[7] Gordon JL, Rubinow DR, Eisenlohr-Moul TA, Xia K, Schmidt PJ, Girdler SS. Efficacy of Transdermal Estradiol and Micronized Progesterone in the Prevention of Depressive Symptoms in the Menopause Transition: A Randomized Clinical Trial. JAMA Psychiatry. 2018 Feb 1;75(2):149-157. doi: 10.1001/jamapsychiatry.2017.3998. PMID: 29322164; PMCID: PMC5838629.
[8]https://www.hopkinsmedicine.org/health/wellness-and-prevention/can-menopause-cause-depression
[9] Masakazu Terauchi,Shiro Hiramitsu, Mihoko Akiyoshi Yoko Owa, Kiyoko Kato
Satoshi Obayashi,Eisuke Matsushima,Toshiro Kubota (2012) Associations between anxiety, depression and insomnia in peri- and post-menopausal women. Maturitas Volume 72, Issue 1, pg 61-65.:https://doi.org/10.1016/j.maturitas.2012.01.014
[10] Bauld, R and Brown, R.F. (2008) Stress, psychological distress, psychosocial factors, menopause symptoms and physical health in women. Maturitas, volume 62, issue 2 p160-165. DOI:https://doi.org/10.1016/j.maturitas.2008.12.00415]
[11] https://www.healthline.com/health/cbt-techniques
[12] Soares CN, Almeida OP, Joffe H, Cohen LS. Efficacy of estradiol for the treatment of depressive disorders in perimenopausal women: a double-blind, randomized, placebo-controlled trial. Arch Gen Psychiatry 2001;58:529-534.
[13] https://www.zrtlab.com/blog/archive/impact-hormones-serotonin-depression/#_edn12
[14] Rybaczyk LA, Bashaw MJ, Pathak DR, Moody SM, Gilders RM, Holzschu DL. An overlooked connection: serotonergic mediation of estrogen-related physiology and pathology. BMC Womens Health. 2005;5:12. Published 2005 Dec 20. doi:10.1186/1472-6874-5-12
[15] https://www.zrtlab.com/blog/archive/mood-menopause-perimenopause